You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Active and Passive InsufficiencyDocument25 pagesActive and Passive Insufficiencydina sharafNo ratings yet
- Anterior Shoulder DislocationDocument2 pagesAnterior Shoulder DislocationcilengsaiNo ratings yet
- Upper Limb MCQsDocument12 pagesUpper Limb MCQsTennyson Machiwenyika91% (11)
- Orthopedic Secrets, 3rd EditionDocument61 pagesOrthopedic Secrets, 3rd EditionPJHG100% (10)
- Biomechanical Analysis of BowlingDocument3 pagesBiomechanical Analysis of BowlingWasemBhat100% (1)
- Rotator Cuff Tear: Basic Understanding and Treatment OptionsDocument26 pagesRotator Cuff Tear: Basic Understanding and Treatment OptionsirsankurniawanNo ratings yet
- Knee PainDocument2 pagesKnee PainKKNo ratings yet
- Ch. 8 Student Packet (ANP)Document5 pagesCh. 8 Student Packet (ANP)Alex ZhangNo ratings yet
- Hip Complex BioDocument18 pagesHip Complex BioVijay PradeepNo ratings yet
- Types of Joints - The Skeleton & Bones - Anatomy & Physiology PDFDocument3 pagesTypes of Joints - The Skeleton & Bones - Anatomy & Physiology PDFPankaj VermaNo ratings yet
- Special Tests For WristDocument13 pagesSpecial Tests For WristSaif Ahmed LariNo ratings yet
- Muscle Grading and Testing Procedures 508 PDFDocument5 pagesMuscle Grading and Testing Procedures 508 PDFNanda Gusmaw BarcellioNo ratings yet
- Exercise: Cristina M. Medina, RN, MAN Jayme P. Hipolito, RN, MAN Lorna Mendoza, RN, MANDocument26 pagesExercise: Cristina M. Medina, RN, MAN Jayme P. Hipolito, RN, MAN Lorna Mendoza, RN, MANAlma Janella TOSINONo ratings yet
- CPPD1Document7 pagesCPPD1Alex GainaNo ratings yet
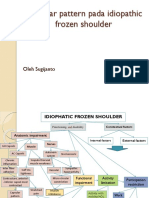
- Capsular Pattern Pada Idiopathic Frozen Shoulder: Oleh SugijantoDocument11 pagesCapsular Pattern Pada Idiopathic Frozen Shoulder: Oleh SugijantoRhany JulyatiNo ratings yet
- Shoulder Rehab Ver2Document7 pagesShoulder Rehab Ver2Daniel Hernandez Tellerias100% (2)
- Hamstring Weakness After Surgery For Anterior Cruciate InjuryDocument4 pagesHamstring Weakness After Surgery For Anterior Cruciate InjuryAdrien VaillatNo ratings yet
- Checklist Hip ExaminationDocument8 pagesChecklist Hip Examinationhakuna matataNo ratings yet
- Cerebral Palsy Special Tests and Corrective ProceduresDocument11 pagesCerebral Palsy Special Tests and Corrective ProceduresOj AlimbuyuguenNo ratings yet
- Summary of Muscles in The ShoulderDocument3 pagesSummary of Muscles in The ShoulderDaniel GraceNo ratings yet
- Orthopedic Assessment Tests Adv Standing Entrance ExamDocument3 pagesOrthopedic Assessment Tests Adv Standing Entrance ExamVahid KhaveNo ratings yet
- Wrist Arthroscopy DuMontierDocument10 pagesWrist Arthroscopy DuMontierjandocNo ratings yet
- Rad Posi Prelim (Sir Mike)Document29 pagesRad Posi Prelim (Sir Mike)Mark Cielo PeraltaNo ratings yet
- To Follow Is A List and Photos Showing Over 100 Exercises That Can Be Performed On Your Bio ForceDocument16 pagesTo Follow Is A List and Photos Showing Over 100 Exercises That Can Be Performed On Your Bio Forcetanweebeng100% (1)
- Shoulder - LectureDocument82 pagesShoulder - LectureElizabethNo ratings yet
- Exercise Rehabilitation in The Non-Operative PDFDocument23 pagesExercise Rehabilitation in The Non-Operative PDFLeonardiniNo ratings yet
- General Anatomy 1 Laboratory: Labelling ReportDocument22 pagesGeneral Anatomy 1 Laboratory: Labelling ReportMigz BolivarNo ratings yet
- MCQsDocument9 pagesMCQsratnav_ratanNo ratings yet
- Hand Tool Project Requirements: The Case of Banana Cultivation and Its Physical Demands (OWAS)Document13 pagesHand Tool Project Requirements: The Case of Banana Cultivation and Its Physical Demands (OWAS)melbe5jane5quiamcoNo ratings yet
- TOSSM-APKASS 2022-ProgramDocument31 pagesTOSSM-APKASS 2022-ProgrampondchoNo ratings yet