You might also like
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsFrom EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsRating: 4.5 out of 5 stars4.5/5 (13)
- Claim Submission ProcedureDocument7 pagesClaim Submission ProcedurePrathameshNo ratings yet
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- Understanding Named, Automatic and Additional Insureds in the CGL PolicyFrom EverandUnderstanding Named, Automatic and Additional Insureds in the CGL PolicyNo ratings yet
- NOC ApplicationDocument17 pagesNOC ApplicationPranilNo ratings yet
- Employment Claims without a Lawyer: A Handbook for Litigants in Person, Revised 2nd editionFrom EverandEmployment Claims without a Lawyer: A Handbook for Litigants in Person, Revised 2nd editionNo ratings yet
- Unihome Care Claim FormDocument2 pagesUnihome Care Claim FormrishiukaiNo ratings yet
- Life, Accident and Health Insurance in the United StatesFrom EverandLife, Accident and Health Insurance in the United StatesRating: 5 out of 5 stars5/5 (1)
- 1S Claimant Statement Form (Health Claims) : 24X7 Customerhelpline No: 1860 266 7766Document5 pages1S Claimant Statement Form (Health Claims) : 24X7 Customerhelpline No: 1860 266 7766basha gNo ratings yet
- A Guide to District Court Civil Forms in the State of HawaiiFrom EverandA Guide to District Court Civil Forms in the State of HawaiiNo ratings yet
- Form ADocument3 pagesForm AhanukohliNo ratings yet
- Claim Submission Checklist - pdf4454101871738174528Document2 pagesClaim Submission Checklist - pdf4454101871738174528Bireswar SamajpatiNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- 3005 Motor Claim Form Perq - 16022023 - Perq 21022023Document5 pages3005 Motor Claim Form Perq - 16022023 - Perq 21022023Bhagya Sri UshanagallaNo ratings yet
- New Claim Form Dhs ReimbursementDocument4 pagesNew Claim Form Dhs Reimbursementamit_bisht2225% (4)
- Claim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Document4 pagesClaim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Boby GanaNo ratings yet
- Monica JainDocument4 pagesMonica Jainx62bzy8pktNo ratings yet
- Domiciliary Claim Form Canara Bank PDFDocument2 pagesDomiciliary Claim Form Canara Bank PDFAnchal katiyarNo ratings yet
- Claim Form Dhs ReimbursementDocument4 pagesClaim Form Dhs ReimbursementrenjithkunnumpurathNo ratings yet
- Claim Submission Procedure for UIIC Group InsuranceDocument7 pagesClaim Submission Procedure for UIIC Group InsuranceAbhishek AswalNo ratings yet
- United India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim FormDocument2 pagesUnited India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim Form'Θκ'βύτ-Ίισνέγσύ.No ratings yet
- Fogg Travel Insurance Medical Expenses Claim FormDocument3 pagesFogg Travel Insurance Medical Expenses Claim FormDiana PanteaNo ratings yet
- 05 - Domiciliary Claim FormDocument2 pages05 - Domiciliary Claim FormSAI SRI VLOGSNo ratings yet
- Easy Health Claim FormDocument4 pagesEasy Health Claim FormQwerty TNo ratings yet
- Easy Health Claim FormDocument4 pagesEasy Health Claim FormAnkithNo ratings yet
- Secure (Personal Accident Insurance Product) Claim FormDocument10 pagesSecure (Personal Accident Insurance Product) Claim Formmestry.om05No ratings yet
- PunitDocument4 pagesPunitx62bzy8pktNo ratings yet
- St. Peter Life Plan Unrendered Service RequirementsDocument3 pagesSt. Peter Life Plan Unrendered Service RequirementsrainrealizoNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Claim Form for Health InsuranceDocument7 pagesClaim Form for Health InsuranceSwapnil NageNo ratings yet
- Genins Claim Form (New)Document3 pagesGenins Claim Form (New)pratikwagh112002No ratings yet
- MediPrime Claim FormDocument8 pagesMediPrime Claim Formrahul0105100% (1)
- Health India TPA - Pre Auth FormDocument5 pagesHealth India TPA - Pre Auth FormBOOKREADER_NOW100% (1)
- 12benefit Payment FormDocument5 pages12benefit Payment Formemmanuelkorli1No ratings yet
- CARE FORM - ReimbuDocument12 pagesCARE FORM - ReimbuPradyumna Singh RathoreNo ratings yet
- Physiomodalities Catlog NewDocument2 pagesPhysiomodalities Catlog NewRKNo ratings yet
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- Claim Report: Travel Insurance Report FormDocument7 pagesClaim Report: Travel Insurance Report Formhoneytrap99No ratings yet
- CLAIM FORM SUBMISSION GUIDEDocument1 pageCLAIM FORM SUBMISSION GUIDEAnonymous W9VINoTza100% (1)
- Claim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument4 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Auser4timepass6237No ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- Ericsson Claim Form PDFDocument2 pagesEricsson Claim Form PDFlovingsayrus100% (1)
- Claim Form - Part ADocument3 pagesClaim Form - Part Agrajesh45No ratings yet
- Form Irda Agents VaDocument2 pagesForm Irda Agents VarenganathanNo ratings yet
- Family Floater Claim FormDocument4 pagesFamily Floater Claim FormSAMNo ratings yet
- SKS Microfinance Employee Hospital Claim FormDocument1 pageSKS Microfinance Employee Hospital Claim FormPiyush MishraNo ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- Personal Accident Critical Illness Hospital Income Claim FormDocument3 pagesPersonal Accident Critical Illness Hospital Income Claim FormHihiNo ratings yet
- Nic Claim FormDocument2 pagesNic Claim FormGopalKrishnaNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- 32805209Document1 page32805209arvindhrmuraliNo ratings yet
- Form No: HI / Claim IntimationDocument2 pagesForm No: HI / Claim IntimationVishal SankheNo ratings yet
- Claim form guideDocument2 pagesClaim form guideSoham BanerjeeNo ratings yet
- UIIC ClaimFormDocument6 pagesUIIC ClaimFormTeja NagetiNo ratings yet
- Personal Accident Claim FormDocument5 pagesPersonal Accident Claim FormMadhava Reddy MunagalaNo ratings yet
- Income Tax Calculator 2010-11Document2 pagesIncome Tax Calculator 2010-11Deepak Kr SinghNo ratings yet
- Personal Accident Claim FormDocument5 pagesPersonal Accident Claim FormMadhava Reddy MunagalaNo ratings yet
- AP Learning License - Telugu FormDocument2 pagesAP Learning License - Telugu FormMadhava Reddy MunagalaNo ratings yet
- Request For New PAN Card Or/ and Changes or Correction in PAN DataDocument4 pagesRequest For New PAN Card Or/ and Changes or Correction in PAN DataMadhava Reddy MunagalaNo ratings yet
- Interpretation of TreatyDocument21 pagesInterpretation of TreatyTania KansalNo ratings yet
- T&C Air BalancingDocument4 pagesT&C Air BalancingAzwan SunlineNo ratings yet
- Institutional Framework FOR International Business: Business R. M. JoshiDocument45 pagesInstitutional Framework FOR International Business: Business R. M. JoshiIshrat SonuNo ratings yet
- Fraud, Internal Controls and Bank ReconciliationDocument15 pagesFraud, Internal Controls and Bank ReconciliationSadia ShithyNo ratings yet
- Sagar Kailas Salunke Primary Account Holder Name: Your A/C StatusDocument3 pagesSagar Kailas Salunke Primary Account Holder Name: Your A/C Statussagar_salunkeNo ratings yet
- Khilafat Movement 1919 1924Document4 pagesKhilafat Movement 1919 1924obaidNo ratings yet
- The Jewish Religion - Chapter 3 - The Talmud and Bible BelieversDocument11 pagesThe Jewish Religion - Chapter 3 - The Talmud and Bible BelieversNatasha MyersNo ratings yet
- s3 UserguideDocument1,167 pagess3 UserguideBetmanNo ratings yet
- NaMo Case StudyDocument4 pagesNaMo Case StudyManish ShawNo ratings yet
- Partnership Liability for Debts IncurredDocument12 pagesPartnership Liability for Debts IncurredDennis VelasquezNo ratings yet
- W-2 Wage and Tax Statement: Copy B-To Be Filed With Employee's FEDERAL Tax ReturnDocument1 pageW-2 Wage and Tax Statement: Copy B-To Be Filed With Employee's FEDERAL Tax ReturnjeminaNo ratings yet
- Deposit Mobilization of Nabil Bank LimitedDocument41 pagesDeposit Mobilization of Nabil Bank Limitedram binod yadav76% (38)
- Jei and Tabligh Jamaat Fundamentalisms-Observed PDFDocument54 pagesJei and Tabligh Jamaat Fundamentalisms-Observed PDFAnonymous EFcqzrdNo ratings yet
- Sentence Correction - English Aptitude MCQ Questions and Answers Page-3 Section-1 - 1603796318303Document4 pagesSentence Correction - English Aptitude MCQ Questions and Answers Page-3 Section-1 - 1603796318303LikeNo ratings yet
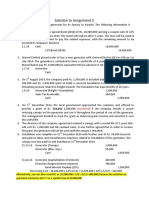
- Assignment 2 SolutionDocument4 pagesAssignment 2 SolutionSobhia Kamal100% (1)
- DuplicateDocument4 pagesDuplicateSakshi ShahNo ratings yet
- Nissan Motors v Secretary of Labor illegal strike rulingDocument2 pagesNissan Motors v Secretary of Labor illegal strike rulingjenellNo ratings yet
- Dispute Credit Report Inaccuracies FormDocument1 pageDispute Credit Report Inaccuracies FormJessica Ashley0% (1)
- Test 1. Answer SheetDocument3 pagesTest 1. Answer SheetAdi AlshtiwiNo ratings yet
- Lucas TVS Price List 2nd May 2011Document188 pagesLucas TVS Price List 2nd May 2011acere18No ratings yet
- Dua Mujeer - LinebylineDocument32 pagesDua Mujeer - LinebylineIsiakaNo ratings yet
- Archipelago of Justice - Law in France's Early Modern EmpireDocument287 pagesArchipelago of Justice - Law in France's Early Modern EmpireaddeNo ratings yet
- Bank StatementDocument2 pagesBank StatementZakaria EL MAMOUNNo ratings yet
- Will NEET PG 2023 Be Postponed Students ApproachDocument1 pageWill NEET PG 2023 Be Postponed Students ApproachBhat MujeebNo ratings yet
- Assurance Services: Definition, Types and LimitationsDocument146 pagesAssurance Services: Definition, Types and LimitationsMudassar Iqbal0% (1)
- Financial Statement: Funds SummaryDocument1 pageFinancial Statement: Funds SummarymorganNo ratings yet
- Perfam Cases 37 UpDocument196 pagesPerfam Cases 37 UpNina IrayNo ratings yet
- Socrates vs. Commission On Elections, G.R. No. 154512 - Case DigestDocument2 pagesSocrates vs. Commission On Elections, G.R. No. 154512 - Case DigestAlena Icao-AnotadoNo ratings yet
- 3000 Watt Power InverterDocument1 page3000 Watt Power InvertersimonNo ratings yet