You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 2011 - Spuriously Raised Serum Creatinine Associated With An Excipient Present in An Intravenous Dexamethasone FormulationDocument4 pages2011 - Spuriously Raised Serum Creatinine Associated With An Excipient Present in An Intravenous Dexamethasone FormulationFede0No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 2015 - Influence of Vitamin K Antagonist Treatment On Activated Partial Thromboplastin TimeDocument4 pages2015 - Influence of Vitamin K Antagonist Treatment On Activated Partial Thromboplastin TimeFede0No ratings yet
- Cerf 74Document13 pagesCerf 74Khawaja WaqasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Oost Erhu Is 2017Document11 pagesOost Erhu Is 2017Fede0No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 2012 - Prediction of The Hematocrit of Dried Blood Spots Via Potassium Measurement On A Routine Clinical Chemistry AnalyzerDocument14 pages2012 - Prediction of The Hematocrit of Dried Blood Spots Via Potassium Measurement On A Routine Clinical Chemistry AnalyzerFede0No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- DBil HemolysisDocument5 pagesDBil HemolysisFede0No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Severinghaus 1986Document14 pagesSeveringhaus 1986Fede0No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Interpretation of Arterial Blood Gas: Review ArticleDocument8 pagesInterpretation of Arterial Blood Gas: Review ArticleFede0No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 2015 - Proteolysis Is A Confounding Factor in The Interpretation of Faecal CalprotectinDocument7 pages2015 - Proteolysis Is A Confounding Factor in The Interpretation of Faecal CalprotectinFede0No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Severing Ha Us 1987Document4 pagesSevering Ha Us 1987Fede0No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 75 FullDocument8 pages75 FullFede0No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 2009 - A New Approach For The Determination of Reference Intervals From Hospital-Based DataDocument6 pages2009 - A New Approach For The Determination of Reference Intervals From Hospital-Based DataFede0No ratings yet
- Decision Making in Clin LabDocument27 pagesDecision Making in Clin LabKelma TayebaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Severinghaus 1986Document16 pagesSeveringhaus 1986Fede0No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Sevenet Et Al-2017-International Journal of Laboratory HematologyDocument8 pagesSevenet Et Al-2017-International Journal of Laboratory HematologyFede0No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shaw 2014Document7 pagesShaw 2014Fede0No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Severing Ha Us 1985Document13 pagesSevering Ha Us 1985Fede0No ratings yet
- 906 Full Hb1acDocument10 pages906 Full Hb1acFede0No ratings yet
- Stubblefield 2012Document8 pagesStubblefield 2012Fede0No ratings yet
- Ball Och 2008sdfDocument8 pagesBall Och 2008sdfFede0No ratings yet
- Ruberto 2017 Clot WaveDocument6 pagesRuberto 2017 Clot WaveFede0No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mechanism of Interference by Hemoglobin in The Determination of Total Bilirubin. II. Method of Jendrassik-GrofDocument4 pagesMechanism of Interference by Hemoglobin in The Determination of Total Bilirubin. II. Method of Jendrassik-GrofFede0No ratings yet
- BMJ h6138 FullDocument10 pagesBMJ h6138 FullFede0No ratings yet
- 10.1016@S0009 89819800164 8Document9 pages10.1016@S0009 89819800164 8Fede0No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 2014 - Physiology and Its Importance For Reference IntervalsDocument12 pages2014 - Physiology and Its Importance For Reference IntervalsFede0No ratings yet
- 2005 - Estimate of Biological Variation of Laboratory Analytes Based On The Third National Health and Nutrition Examination SurveyDocument3 pages2005 - Estimate of Biological Variation of Laboratory Analytes Based On The Third National Health and Nutrition Examination SurveyFede0No ratings yet
- 2010 - Estimating Reference IntervalsDocument3 pages2010 - Estimating Reference IntervalsFede0No ratings yet
- 2009 - Reference Intervals The Way ForwardDocument11 pages2009 - Reference Intervals The Way ForwardFede0No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- 2000 - Hematological Health-Related Intervals Estimated Using An Indirect Method in Order To Satisfy The Accreditation StandardsDocument4 pages2000 - Hematological Health-Related Intervals Estimated Using An Indirect Method in Order To Satisfy The Accreditation StandardsFede0No ratings yet
- Disseminated Intravascular Coagulation in Paediatrics: Revathi Rajagopal, Jecko Thachil, Paul MonagleDocument8 pagesDisseminated Intravascular Coagulation in Paediatrics: Revathi Rajagopal, Jecko Thachil, Paul MonagleRizky LumalessilNo ratings yet
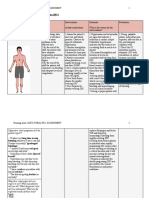
- Nursing Clients With Hematologic DisordersDocument4 pagesNursing Clients With Hematologic DisordersLuna MarieNo ratings yet
- Metabolic Encephalopathies in The Critical Care Unit: Review ArticleDocument29 pagesMetabolic Encephalopathies in The Critical Care Unit: Review ArticleFernando Dueñas MoralesNo ratings yet
- Chapter Review: True or FalseDocument2 pagesChapter Review: True or FalseJames Gabriel SalardaNo ratings yet
- Bleeding Time, Clotting Time PT and PTT2Document41 pagesBleeding Time, Clotting Time PT and PTT2Qurrataini Ibanez100% (1)
- Shock Hemorrágico PDFDocument10 pagesShock Hemorrágico PDFMillerAponteNo ratings yet
- Rash BookDocument12 pagesRash BookPhoebe UsmleNo ratings yet
- Assessment of Platelet Numbers and Morphology in The Peripheral Blood SmearDocument21 pagesAssessment of Platelet Numbers and Morphology in The Peripheral Blood SmearanggaririnNo ratings yet
- Golpe de Calor NEJMDocument11 pagesGolpe de Calor NEJMJair Alexander Quintero PanucoNo ratings yet
- TP4Document14 pagesTP4Asdfghjl0% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PBM Module1 MTP Template 0Document2 pagesPBM Module1 MTP Template 01234chocoNo ratings yet
- Chilblain MicroangiopathyDocument6 pagesChilblain MicroangiopathytitoNo ratings yet
- Care of The Clients With Cancer: Prof. Hashim N. Alawi Jr. RN, MANDocument78 pagesCare of The Clients With Cancer: Prof. Hashim N. Alawi Jr. RN, MANjisooNo ratings yet
- All Obgyn Osce (2) Good Book For OsceDocument75 pagesAll Obgyn Osce (2) Good Book For OsceMohamed Hassan91% (47)
- Exercise No. 26 The Blood GroupsDocument8 pagesExercise No. 26 The Blood GroupsPATRICIA ROSE SORIANONo ratings yet
- Obstetric Nursing DrillsDocument14 pagesObstetric Nursing DrillsClarence AnescoNo ratings yet
- Anticoagulants, Fibrinolytics, AntiplateletsDocument88 pagesAnticoagulants, Fibrinolytics, Antiplateletspmuawiyah25No ratings yet
- Hematology 2 Lecture Notes Platelet Quantitative DisordersDocument10 pagesHematology 2 Lecture Notes Platelet Quantitative DisorderscccomayogNo ratings yet
- Disorders of HemostasisDocument50 pagesDisorders of Hemostasisalibayaty1100% (1)
- Hemostasis Basics Programmed Learner: TopicDocument19 pagesHemostasis Basics Programmed Learner: TopicAahsan Iqbal احسن اقبالNo ratings yet
- DIC Case StudyDocument3 pagesDIC Case StudyJuliaNo ratings yet
- Oncology NotesDocument7 pagesOncology Notesaurezea100% (1)
- Dengue Hemorrhagic Fever With Disseminated Intravascular CoagulationDocument2 pagesDengue Hemorrhagic Fever With Disseminated Intravascular CoagulationPutriPasaribuNo ratings yet
- Rodaks Hema 2 Lec Chapter 39&40Document45 pagesRodaks Hema 2 Lec Chapter 39&40Ivory Mae Verona AndayaNo ratings yet
- Electrical Burn PathophysiologyDocument1 pageElectrical Burn PathophysiologydanicaNo ratings yet
- Soluble Fibrin AssaysDocument34 pagesSoluble Fibrin AssaysAndo KillingmeinsideNo ratings yet
- Antepartum HaemorrhageDocument65 pagesAntepartum HaemorrhageAmit RamrattanNo ratings yet
- Oncology NursingDocument12 pagesOncology NursingDick Morgan Ferrer80% (5)
- Chapter 33 - Assessment and Management of Patients With HematologicDocument8 pagesChapter 33 - Assessment and Management of Patients With HematologicMichael Boado100% (1)
- Module 10 Student Activity SheetDocument7 pagesModule 10 Student Activity SheetJenny Agustin FabrosNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)