You might also like
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z96% (26)
- RespiratoryDocument4 pagesRespiratoryHaliana IzatiNo ratings yet
- Pulse OximetryDocument38 pagesPulse OximetryJoanna Jauculan Albaño100% (2)
- @anesthesia Books 2021 The Complete Recovery Room Book 6th EditionDocument601 pages@anesthesia Books 2021 The Complete Recovery Room Book 6th EditionName correo100% (2)
- Comprehens Ive Nursing Care On CabgDocument25 pagesComprehens Ive Nursing Care On CabgRizwan BelimNo ratings yet
- Cardio MCQDocument9 pagesCardio MCQtheonlymehul100% (2)
- Pediatric Septic ShockDocument24 pagesPediatric Septic ShockBRENDA AMARONo ratings yet
- ShockDocument30 pagesShockvinnu kalyanNo ratings yet
- Psikometric ChartDocument1 pagePsikometric Chartjohn_kadier651No ratings yet
- Bureau Veritas Leading Provider Quality Assurance ServicesDocument7 pagesBureau Veritas Leading Provider Quality Assurance ServicesAnonyNo ratings yet
- Af Prevention CHFDocument4 pagesAf Prevention CHFDewi AyuNo ratings yet
- Bod Cerebrovasculardiseasestroke PDFDocument67 pagesBod Cerebrovasculardiseasestroke PDFMax Laban SeminarioNo ratings yet
- Bod CerebrovasculardiseasestrokeDocument67 pagesBod CerebrovasculardiseasestrokeErlin IrawatiNo ratings yet
- Global Burden of Cerebrovascular DiseaseDocument67 pagesGlobal Burden of Cerebrovascular DiseasederiNo ratings yet
- Early Repolarization Pattern and Risk For Arrhythmia Death Meta AnalysisDocument6 pagesEarly Repolarization Pattern and Risk For Arrhythmia Death Meta Analysisfindingnemo667No ratings yet
- Left Atrial Volume Predicts Cardiovascular EventsDocument6 pagesLeft Atrial Volume Predicts Cardiovascular EventsWirawan PrabowoNo ratings yet
- Blood Pressure Control and Primary Prevention of Stroke: Summary of The Recent Clinical Trial Data and Meta-AnalysesDocument16 pagesBlood Pressure Control and Primary Prevention of Stroke: Summary of The Recent Clinical Trial Data and Meta-AnalysesAngelika AHuiNo ratings yet
- Mitral Valve Prolapse Prevalence and Complications: An Ongoing DialogueDocument4 pagesMitral Valve Prolapse Prevalence and Complications: An Ongoing Dialoguemaya damayantiNo ratings yet
- Faktor Resiko Utama Gagal JantungDocument8 pagesFaktor Resiko Utama Gagal Jantungaxl___No ratings yet
- Hendro Susilo-Af and StrokeDocument7 pagesHendro Susilo-Af and StrokeyudisNo ratings yet
- Estudio FraminghamDocument7 pagesEstudio FraminghamJulio FloresNo ratings yet
- Syncope in Adults - Epidemiology, Pathogenesis, and EtiologiesDocument28 pagesSyncope in Adults - Epidemiology, Pathogenesis, and EtiologiesRaúl MartínezNo ratings yet
- Effect of Left Ventricular Outflow Tract Obstruction On Clinical Outcome in Hypertrophic CardiomyopathyDocument9 pagesEffect of Left Ventricular Outflow Tract Obstruction On Clinical Outcome in Hypertrophic CardiomyopathyAstrid Noviera IksanNo ratings yet
- JAH3 5 E003347Document13 pagesJAH3 5 E003347AllahbesertkitaNo ratings yet
- Etiologji Dhe Epidemiologjia e StrokeDocument7 pagesEtiologji Dhe Epidemiologjia e StrokegranitNo ratings yet
- Prevalensi Sindrom Koroner Akut Di RSUP Prof. Dr. R. D. Kandou Manado Periode 1 Januari 2014 - 31 Desember 2014Document8 pagesPrevalensi Sindrom Koroner Akut Di RSUP Prof. Dr. R. D. Kandou Manado Periode 1 Januari 2014 - 31 Desember 2014lulukNo ratings yet
- Prevalence of Ventricular Arrhythmia and Its Associated Factors in Nondialyzed Chronic Kidney Disease PatientsDocument8 pagesPrevalence of Ventricular Arrhythmia and Its Associated Factors in Nondialyzed Chronic Kidney Disease Patientsjustin_saneNo ratings yet
- Stroke Epidemiology: Advancing Our Understanding of Disease Mechanism and TherapyDocument12 pagesStroke Epidemiology: Advancing Our Understanding of Disease Mechanism and TherapyDodik's NihNo ratings yet
- The Effects of Heart Failure On Renal FunctionDocument16 pagesThe Effects of Heart Failure On Renal FunctionNurul KamajayaNo ratings yet
- Atrial Fibrillation ElderlyDocument18 pagesAtrial Fibrillation ElderlyRESIDENTES MEDICINA INTERNANo ratings yet
- Acute Ischemic Stroke UpdateDocument38 pagesAcute Ischemic Stroke Updatenarendra wahyuNo ratings yet
- And Recurrence Ischemic Stroke Subtypes: A Population-Based Study of Functional Outcome, SurvivalDocument8 pagesAnd Recurrence Ischemic Stroke Subtypes: A Population-Based Study of Functional Outcome, SurvivalBeningPutriRamadhaniUsmanNo ratings yet
- Epidemiology of and Risk Factors For Atrial Fibrillation - UpToDateDocument22 pagesEpidemiology of and Risk Factors For Atrial Fibrillation - UpToDateAarash Habibi100% (1)
- Time Trends in The Prevalence of Atherosclerosis: A Population-Based Autopsy Study in March 2011Document5 pagesTime Trends in The Prevalence of Atherosclerosis: A Population-Based Autopsy Study in March 2011iamjenivicNo ratings yet
- NIH Public AccessDocument16 pagesNIH Public AccessaudiNo ratings yet
- Definition, Epidemiology, and Prognosis: Reproduced With Permission From The AHADocument10 pagesDefinition, Epidemiology, and Prognosis: Reproduced With Permission From The AHAIboy ZulhamNo ratings yet
- Ni Hms 643292Document12 pagesNi Hms 643292LeksmanaHidayatullahNo ratings yet
- Guidelines For The Management of Patients With Unruptured Intracranial AneurysmsDocument60 pagesGuidelines For The Management of Patients With Unruptured Intracranial AneurysmskvintumbelNo ratings yet
- Vascular risk factors may prevent dementiaDocument11 pagesVascular risk factors may prevent dementiabdalcin5512No ratings yet
- Management of Ischaemic Stroke2000Document29 pagesManagement of Ischaemic Stroke2000FEllis LEoNo ratings yet
- Joc15132 2120 2127Document8 pagesJoc15132 2120 2127caio personalNo ratings yet
- Peripheral Artery Disease: Clinical PracticeDocument11 pagesPeripheral Artery Disease: Clinical Practiceapi-311409998No ratings yet
- Captura de Pantalla 2021-08-02 A La(s) 1.24.53 P. M.Document6 pagesCaptura de Pantalla 2021-08-02 A La(s) 1.24.53 P. M.Andres Felipe Quimbayo CifuentesNo ratings yet
- Jurnal RinkeDocument8 pagesJurnal RinkeRaka AqbarNo ratings yet
- Anticoagulant Therapy For Ischemic StrokeDocument6 pagesAnticoagulant Therapy For Ischemic StrokeDewi LestariNo ratings yet
- BrochureDocument2 pagesBrochureapi-272621489No ratings yet
- HHS Public AccessDocument13 pagesHHS Public AccessArdian PratiaksaNo ratings yet
- 30 58 1 PBDocument7 pages30 58 1 PBTopheng UmagaphyNo ratings yet
- Abstracs Neuroepidemiology 2021Document106 pagesAbstracs Neuroepidemiology 2021NICOLAS PEREZNo ratings yet
- Acute Coronary SyndromesDocument1 pageAcute Coronary SyndromesSherZalattha KuchikiElfNo ratings yet
- Gastroenteritis Outbreak Tied To Later Health Problems: HealthdayDocument5 pagesGastroenteritis Outbreak Tied To Later Health Problems: HealthdayJammae RubillosNo ratings yet
- Epidemiology of Coronary Heart Disease and Acute Coronary SyndromeDocument6 pagesEpidemiology of Coronary Heart Disease and Acute Coronary SyndromeAnonymous GpgioaDAbNo ratings yet
- Blood Pressure and Clinical Outcomes in The International Stroke TrialDocument7 pagesBlood Pressure and Clinical Outcomes in The International Stroke TrialMif Al-HudaNo ratings yet
- Psychology of Women 401 807Document407 pagesPsychology of Women 401 807Alessio TinerviaNo ratings yet
- Usefulness of Diabetes Mellitus To Predict Long-Term Outcomes in Patients With Unstable Angina Pectoris.Document15 pagesUsefulness of Diabetes Mellitus To Predict Long-Term Outcomes in Patients With Unstable Angina Pectoris.Diah Kris AyuNo ratings yet
- Sudden DeathDocument11 pagesSudden DeathhompalahompalaNo ratings yet
- Study of Pattern of Acute Myocardial Infarction in Tertiary Care Hospital of Ahmedabad, GujaratDocument6 pagesStudy of Pattern of Acute Myocardial Infarction in Tertiary Care Hospital of Ahmedabad, GujaratEditor_IAIMNo ratings yet
- Stroke IskemikDocument49 pagesStroke IskemikyasserNo ratings yet
- A Prospective Study of Sudden Cardiac JournalDocument9 pagesA Prospective Study of Sudden Cardiac JournalRio Andika AbdullahNo ratings yet
- Study of Various Cardiac Arrhythmias in Patients of Acute Myocardial InfarctionDocument10 pagesStudy of Various Cardiac Arrhythmias in Patients of Acute Myocardial InfarctionEditor_IAIMNo ratings yet
- 1 PBDocument10 pages1 PBipan ferrelNo ratings yet
- Stroke 2011 Schäbitz 2385 6Document3 pagesStroke 2011 Schäbitz 2385 6Amry Irsyada YusufNo ratings yet
- The Role of Genetic Variation in Haemorrhagic Stroke: An UpdateDocument4 pagesThe Role of Genetic Variation in Haemorrhagic Stroke: An UpdateLulu LuwiiNo ratings yet
- Heart Kidney InteractionDocument11 pagesHeart Kidney InteractionMichael HostiadiNo ratings yet
- 2011 Cardiovascular Disease Prevention in WomenDocument20 pages2011 Cardiovascular Disease Prevention in WomenRafi UllahNo ratings yet
- Sudden Death in Young AdultsDocument11 pagesSudden Death in Young AdultsdokteralmisrunNo ratings yet
- WASID Trial 2005Document12 pagesWASID Trial 2005cristhian_carvaja_13No ratings yet
- Prevention of Stroke in Patients With Silent Cerebrovascular DiseaseDocument35 pagesPrevention of Stroke in Patients With Silent Cerebrovascular DiseaseparackalphilipNo ratings yet
- Gender Differences in the Pathogenesis and Management of Heart DiseaseFrom EverandGender Differences in the Pathogenesis and Management of Heart DiseaseNo ratings yet
- Manual of Outpatient CardiologyFrom EverandManual of Outpatient CardiologyJohn D. BisognanoNo ratings yet
- Neurological Sudden Death Is Not Rare: Anthony L. Komaroff, MDDocument2 pagesNeurological Sudden Death Is Not Rare: Anthony L. Komaroff, MDAnonyNo ratings yet
- Neurological Sudden Death Is Not Rare: Anthony L. Komaroff, MDDocument2 pagesNeurological Sudden Death Is Not Rare: Anthony L. Komaroff, MDAnonyNo ratings yet
- Insert Fields in Word - Office SupportDocument13 pagesInsert Fields in Word - Office SupportAnonyNo ratings yet
- Trick With MS WordsDocument19 pagesTrick With MS WordsAnonyNo ratings yet
- Neurological Sudden Death Is Not Rare: Anthony L. Komaroff, MDDocument2 pagesNeurological Sudden Death Is Not Rare: Anthony L. Komaroff, MDAnonyNo ratings yet
- Action Verbs For ResumesDocument2 pagesAction Verbs For Resumesapi-2627751040% (1)
- Sucess in Africa S Energy Sector PDFDocument2 pagesSucess in Africa S Energy Sector PDFAnonyNo ratings yet
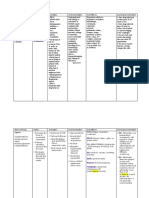
- Name of Drug Action Indication Contraindication Side Effects Nursing Consideration AspirinDocument5 pagesName of Drug Action Indication Contraindication Side Effects Nursing Consideration AspirinPerpetual DaltaNo ratings yet
- Excretory System Anatomy and Physiology LabDocument4 pagesExcretory System Anatomy and Physiology LabChrista Villanueva MalinaoNo ratings yet
- HYPERTENSION-WPS OfficeDocument4 pagesHYPERTENSION-WPS OfficeAMOS MELINo ratings yet
- 9-Andre Tan - S Surgical NotesDocument163 pages9-Andre Tan - S Surgical Notes肖楚天No ratings yet
- HepatomegalyDocument1 pageHepatomegalywounded86100% (1)
- L75 - Pathology of CNS TumorsDocument73 pagesL75 - Pathology of CNS Tumorsb deepthiNo ratings yet
- Case Write-Up 2Document22 pagesCase Write-Up 2Syed TalhaNo ratings yet
- St. Luke's College of Medicine Cognitive and Mental Disorders LectureDocument8 pagesSt. Luke's College of Medicine Cognitive and Mental Disorders LectureDane Mikhael CalicaNo ratings yet
- Midwives Exemptions PolicyDocument23 pagesMidwives Exemptions Policykerriesha dacresNo ratings yet
- Organ Systems OverviewDocument4 pagesOrgan Systems OverviewdivineNo ratings yet
- Keros Corporate Presentation Jan'24Document49 pagesKeros Corporate Presentation Jan'24hrshtnainwalNo ratings yet
- Ebook Dental Hygiene Theory and Practice 4Th Edition Leonardi Test Bank Full Chapter PDFDocument31 pagesEbook Dental Hygiene Theory and Practice 4Th Edition Leonardi Test Bank Full Chapter PDFsauflyallowerrf1qs100% (8)
- Istilah Kode Icd 9-10Document218 pagesIstilah Kode Icd 9-10nurlinda hafizaNo ratings yet
- Nervous System Lesson 1Document7 pagesNervous System Lesson 1Yennifer NivarNo ratings yet
- Ninja - Antianginal Drugs PDFDocument2 pagesNinja - Antianginal Drugs PDFErica Hyeyeon LeeNo ratings yet
- Anatomy of Cardio Vascular System NotesDocument16 pagesAnatomy of Cardio Vascular System NotesAgleema AhmedNo ratings yet
- Cardiac Markers-101Document35 pagesCardiac Markers-101Rogue Moniker100% (1)
- Jejunum IleumDocument55 pagesJejunum IleumDitas ChuNo ratings yet
- Drug Study: Aspirin (Asa)Document5 pagesDrug Study: Aspirin (Asa)Shara Lailanie A. AzisNo ratings yet
- Cardio Quiz For NSG 128 HDocument22 pagesCardio Quiz For NSG 128 HMac MacapilNo ratings yet
- Thesis Shourya PPT 2 3Document24 pagesThesis Shourya PPT 2 3Y ShouryaNo ratings yet
- Endo ReviewerDocument5 pagesEndo ReviewerZIAN LABADIANo ratings yet