You might also like
- My Bar Exam Journey PDFDocument9 pagesMy Bar Exam Journey PDFJC ComonNo ratings yet
- Beyond Words SatchidanandaDocument194 pagesBeyond Words Satchidanandamjoseyoga86% (7)
- Perdev Q3 M1Document18 pagesPerdev Q3 M1Sally GargaceranNo ratings yet
- Likert ScaleDocument5 pagesLikert ScaleCART11No ratings yet
- Field Trip WaiverDocument1 pageField Trip WaiverNolram LeuqarNo ratings yet
- PersuasionDocument49 pagesPersuasionJeremy Alexander100% (3)
- CS Form No. 212 Personal Data Sheet RevisedDocument4 pagesCS Form No. 212 Personal Data Sheet RevisedJean Castro76% (106)
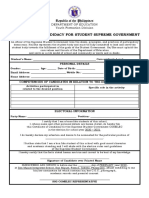
- Certificate of Candidacy and Parental ConsentDocument2 pagesCertificate of Candidacy and Parental ConsentGilbert Quilang Ridao100% (4)
- Work Immersion AppraisalDocument6 pagesWork Immersion AppraisalNathaniel RectoNo ratings yet
- (Guia Reluya) Application Letter - Registration Officer IDocument1 page(Guia Reluya) Application Letter - Registration Officer IGuiaReluya100% (1)
- Letter of Intent To Re Apply For A Job SampleDocument1 pageLetter of Intent To Re Apply For A Job SampleValentin CiorobaNo ratings yet
- Omnibus Certification DepEd Nueva VizcayaDocument1 pageOmnibus Certification DepEd Nueva VizcayaMaria Victoria PadroNo ratings yet
- Example Commission On Election Authorization LetterDocument1 pageExample Commission On Election Authorization LetterArianne De Castro100% (2)
- Republic Act No. 7877Document4 pagesRepublic Act No. 7877PingotMaganga100% (1)
- Fun Run Event WaiverDocument1 pageFun Run Event WaiverAnonymous 6AM6dyNSNo ratings yet
- Parental Consent and Waiver Form Outreach ProgramDocument2 pagesParental Consent and Waiver Form Outreach ProgramNastasia Besin100% (1)
- Nudge - by ThalerDocument7 pagesNudge - by ThalerRaluca Frumuselu80% (5)
- Mou Work ImmersionDocument6 pagesMou Work ImmersionMarlou GayaneloNo ratings yet
- 2015 SALN FormDocument4 pages2015 SALN Formwyclef_chin100% (6)
- Abs CBN Vs Director of Bureau of TrademarksDocument3 pagesAbs CBN Vs Director of Bureau of Trademarkskristel jane caldozaNo ratings yet
- Abs CBN Vs Director of Bureau of TrademarksDocument3 pagesAbs CBN Vs Director of Bureau of Trademarkskristel jane caldozaNo ratings yet
- Letter Request For Dr. DuhaylungsodDocument1 pageLetter Request For Dr. DuhaylungsodYong Rosabal100% (1)
- 6 Attendance SheetDocument1 page6 Attendance SheetRoldan Agad Saren100% (2)
- Eastern and Australian Steamship Co., LTD vs. Great American Insurance Co.Document2 pagesEastern and Australian Steamship Co., LTD vs. Great American Insurance Co.Herazeus UyNo ratings yet
- 20 Macasaet V PeopleDocument2 pages20 Macasaet V PeopleKeisha Mariah Catabay Lauigan100% (1)
- LESSON 3 FS 1 CHAPTER 6.editedDocument6 pagesLESSON 3 FS 1 CHAPTER 6.editedJanine Binbing100% (2)
- Dual Process Theories in Moral PsychologyDocument422 pagesDual Process Theories in Moral PsychologyMaria Beatrice100% (1)
- Escheat: Research Paper On Remedial Law Review Rule 91-EscheatsDocument3 pagesEscheat: Research Paper On Remedial Law Review Rule 91-EscheatsJC ComonNo ratings yet
- Omnibus Certification - Public School TeachersDocument2 pagesOmnibus Certification - Public School Teachersceejaye94% (54)
- Work Immersion - Training Agreement and Liability WaiverDocument2 pagesWork Immersion - Training Agreement and Liability WaiverSteve Marville Aguinaldo50% (2)
- Letter of PermissionDocument2 pagesLetter of PermissionJM Capinig100% (1)
- Board ResolutionDocument2 pagesBoard ResolutionMark MarasiganNo ratings yet
- AUTHORIZATION LETTER For LBCDocument2 pagesAUTHORIZATION LETTER For LBCJanna Fabia100% (1)
- Republic Act No 3571Document15 pagesRepublic Act No 3571Julian Duba100% (2)
- Letter of ReinstatementDocument1 pageLetter of ReinstatementMyung DaeNo ratings yet
- Preschool Contract DepED Gonzaga West DistrictDocument2 pagesPreschool Contract DepED Gonzaga West DistrictJeferson SardengNo ratings yet
- Filing of Candidacy PacketDocument8 pagesFiling of Candidacy PacketFrancis Louie MendozaNo ratings yet
- Certification No Conflict of InterestDocument1 pageCertification No Conflict of InterestRia Tiglao Fortugaliza75% (4)
- Letter of IntentDocument1 pageLetter of IntentCarmellet Lalas100% (1)
- Criteria For Judging 2017Document3 pagesCriteria For Judging 2017Sui Ge Neris100% (1)
- Rada v. NLRC (Digest)Document2 pagesRada v. NLRC (Digest)Jewelito de Guzman0% (1)
- TVL Classes Work Immersion Program Parental Consent: Tulay Na Lupa National High SchoolDocument1 pageTVL Classes Work Immersion Program Parental Consent: Tulay Na Lupa National High SchoolAloc MavicNo ratings yet
- Oesmer Vs Paraiso Dev T CorpDocument2 pagesOesmer Vs Paraiso Dev T CorpKling KingNo ratings yet
- Authorization Letter TORDocument1 pageAuthorization Letter TORmsannrivera100% (3)
- Letter of Intent For Conducting A Feeeding ProgramDocument1 pageLetter of Intent For Conducting A Feeeding ProgramJunard Asentista100% (2)
- Authorization For PSADocument1 pageAuthorization For PSAJAY CADAY0% (2)
- Excuse Letter - UndertimeDocument1 pageExcuse Letter - UndertimeChambee Chambee100% (3)
- Quilala LecturesDocument33 pagesQuilala LecturesJC ComonNo ratings yet
- SSG Letter Pass The HatDocument1 pageSSG Letter Pass The HatJoseph Mark Baldomar100% (1)
- Activity ProposalDocument2 pagesActivity ProposalJunior HumorNo ratings yet
- Authorization LetterDocument1 pageAuthorization LetterEdzNavarroNo ratings yet
- Sample Endorsement LetterDocument1 pageSample Endorsement LetterMark Charle Mana IINo ratings yet
- Cleaning Monitoring FormDocument1 pageCleaning Monitoring FormRoxanne Madugay D. GanoNo ratings yet
- Palisoc DoctrineDocument11 pagesPalisoc Doctrinegurongkalbo0% (1)
- Sportsfest CS Tryouts WaiverDocument2 pagesSportsfest CS Tryouts WaiverRia Pamintuan Quinagutan100% (1)
- 117 BPI Vs Casa Montessori International and Leonardo T. Yabut GR 149454Document1 page117 BPI Vs Casa Montessori International and Leonardo T. Yabut GR 149454Alan GultiaNo ratings yet
- Certificate of AppearanceDocument3 pagesCertificate of AppearanceLoraine AnnaNo ratings yet
- 2015 WB Badminton Tourney Solicitation LetterDocument2 pages2015 WB Badminton Tourney Solicitation LetterRL N DeiparineNo ratings yet
- OJT WaiverDocument1 pageOJT WaiverJames Louis Barcenas100% (1)
- Parents Waiver 2019 2020Document1 pageParents Waiver 2019 2020Keil Morada100% (2)
- Affidavit/Sworn Statement of Actual Care and Custody: (Signature Over Printed Name) (Signature Over Printed Name)Document2 pagesAffidavit/Sworn Statement of Actual Care and Custody: (Signature Over Printed Name) (Signature Over Printed Name)Jojo JojoNo ratings yet
- Dccco Loan FormDocument2 pagesDccco Loan FormJane CA100% (3)
- Sworn Declaration of Relatives EARLDocument1 pageSworn Declaration of Relatives EARLEarl Young100% (1)
- Indorsement TemplateDocument2 pagesIndorsement TemplateJosephine Aya50% (4)
- Schools Omnibus Certificate of Compliance: Depedro13-Rec-004/R3/2-18-2020Document2 pagesSchools Omnibus Certificate of Compliance: Depedro13-Rec-004/R3/2-18-2020Center for Healthcare ProfessionsNo ratings yet
- OMNIBUSDocument6 pagesOMNIBUSCindy Jauculan100% (1)
- Application For Completion of Grades For Under GraduatesDocument1 pageApplication For Completion of Grades For Under GraduatesJoann Saballero Hamili100% (2)
- Work Immersion LetterDocument3 pagesWork Immersion LetterGlenda Mae AlmodielNo ratings yet
- Sample MemoDocument1 pageSample MemoCamille LopezNo ratings yet
- Waiver ConvergeDocument2 pagesWaiver ConvergeMary Ann Amparo0% (1)
- Certificate of EmploymentDocument1 pageCertificate of EmploymentGlenda PaduaNo ratings yet
- Excuse LetterDocument2 pagesExcuse LetterJanice Sapin LptNo ratings yet
- Coastal Clean UpDocument1 pageCoastal Clean UpAnonymous sgEtt4No ratings yet
- Volleyball WaiverDocument1 pageVolleyball Waivernsidney100% (1)
- City Hall, Malabon General Trias, CaviteDocument1 pageCity Hall, Malabon General Trias, CaviteDon NicksNo ratings yet
- Job Order Application LetterDocument1 pageJob Order Application LetterRheem Quiroga100% (1)
- Natcon Parental Consent and WaiverDocument2 pagesNatcon Parental Consent and WaiverReyo VillanuevaNo ratings yet
- Student Registration Form: Student Health & Diet InformationDocument2 pagesStudent Registration Form: Student Health & Diet InformationteacherdarNo ratings yet
- School WaiverDocument3 pagesSchool WaiverMarlon SolanoNo ratings yet
- Details For CADocument1 pageDetails For CAJC ComonNo ratings yet
- Qkrsjfli Qkrsjfli Qrjpkrty Qrjpkrty Ukeurdty Ukeurdty Let Let S.L. S.L. 1 ?) 1 ?)Document9 pagesQkrsjfli Qkrsjfli Qrjpkrty Qrjpkrty Ukeurdty Ukeurdty Let Let S.L. S.L. 1 ?) 1 ?)JC ComonNo ratings yet
- Jurists Bar Review Center: 2020-2021 Schedule of Online Pre-Bar Lectures and ActivitiesDocument4 pagesJurists Bar Review Center: 2020-2021 Schedule of Online Pre-Bar Lectures and ActivitiesYuri AnnNo ratings yet
- Bar Guide: MaterialsDocument6 pagesBar Guide: MaterialsJC ComonNo ratings yet
- Electronic EvidenceDocument10 pagesElectronic EvidenceJC ComonNo ratings yet
- How To Run Game!!Document1 pageHow To Run Game!!JC ComonNo ratings yet
- The Stay Order of The Rehabilitation CourtDocument3 pagesThe Stay Order of The Rehabilitation CourtJC ComonNo ratings yet
- Escheat: Research Paper On Remedial Law Review Rule 91-EscheatsDocument4 pagesEscheat: Research Paper On Remedial Law Review Rule 91-EscheatsJC ComonNo ratings yet
- 2019 Civ Bar QADocument22 pages2019 Civ Bar QAJC ComonNo ratings yet
- The Stay Order of The Rehabilitation CourtDocument3 pagesThe Stay Order of The Rehabilitation CourtJC ComonNo ratings yet
- Corporation Code Outline 4Document31 pagesCorporation Code Outline 4JC ComonNo ratings yet
- Electronic EvidenceDocument10 pagesElectronic EvidenceJC ComonNo ratings yet
- Escheat: Research Paper On Remedial Law Review Rule 91-EscheatsDocument4 pagesEscheat: Research Paper On Remedial Law Review Rule 91-EscheatsJC ComonNo ratings yet
- Petitioner vs. VS.: Second DivisionDocument13 pagesPetitioner vs. VS.: Second Divisionmceline19No ratings yet
- SBCA Legal Forms SeatWork 4-14-18Document1 pageSBCA Legal Forms SeatWork 4-14-18JC ComonNo ratings yet
- Swidler and Berlin v. U.S DecisionDocument11 pagesSwidler and Berlin v. U.S DecisionArla AgrupisNo ratings yet
- Guy Vs Ca Facts:: Civpro April 18 - Abasta - Dy - Federico - Ricaplaza 1Document25 pagesGuy Vs Ca Facts:: Civpro April 18 - Abasta - Dy - Federico - Ricaplaza 1JC ComonNo ratings yet
- Petitioners Vs Vs Respondent: Third DivisionDocument9 pagesPetitioners Vs Vs Respondent: Third DivisionJC ComonNo ratings yet
- San Beda College Alabang School of LawDocument2 pagesSan Beda College Alabang School of LawJC ComonNo ratings yet
- Pathology-0909I-Common Tropical Infections of The CVSDocument10 pagesPathology-0909I-Common Tropical Infections of The CVSJC ComonNo ratings yet
- Police Report2Document2 pagesPolice Report2JC ComonNo ratings yet
- Villanueva L. SEMDocument3 pagesVillanueva L. SEMJC ComonNo ratings yet
- Iv. Doctrine of Corporate Entity A. Doctrine/ Effects:: BUSORG2 OUTLINE 2 (2018) Prof. MIP RomeroDocument1 pageIv. Doctrine of Corporate Entity A. Doctrine/ Effects:: BUSORG2 OUTLINE 2 (2018) Prof. MIP RomeroJC ComonNo ratings yet
- Laval S. Wilson Moved His Rochester Problems To BostonDocument2 pagesLaval S. Wilson Moved His Rochester Problems To BostonSyndicated NewsNo ratings yet
- Models & Theories of PRDocument37 pagesModels & Theories of PRPriyanshi jainNo ratings yet
- Development of Moral CharacterDocument24 pagesDevelopment of Moral CharacterLara Kaye Ganas ValenciaNo ratings yet
- Persons and Family Relations - CasesDocument167 pagesPersons and Family Relations - CasesBethany Divine JimenezNo ratings yet
- People of The Philippines vs. Floro Barcela G.R. No. 208760 April 23, 2014 Mendoza, J.: FactsDocument10 pagesPeople of The Philippines vs. Floro Barcela G.R. No. 208760 April 23, 2014 Mendoza, J.: FactsL.A.No ratings yet
- Syllabus 2011Document16 pagesSyllabus 2011Chong CpmNo ratings yet
- Catherine Liason Lesson ObservationDocument2 pagesCatherine Liason Lesson Observationapi-471129422No ratings yet
- Susan WolfDocument22 pagesSusan WolfKyle ScottNo ratings yet
- Hazrat Ali QuotationsDocument11 pagesHazrat Ali QuotationsM HABIBULLAHNo ratings yet
- Lawsuit Against Leon Valley PDFDocument45 pagesLawsuit Against Leon Valley PDFDavid IbanezNo ratings yet
- Sustainable DevelopmentDocument41 pagesSustainable Developmentnithiamrita0% (3)
- Philosophical Trends in The Feminist MovementDocument22 pagesPhilosophical Trends in The Feminist MovementMahatma GandhiNo ratings yet
- Crossover? Be Strong and Courageous: IntroductionsDocument3 pagesCrossover? Be Strong and Courageous: IntroductionsPaulDanielDeLeonNo ratings yet
- LESSON 1 Theories of Philippine PoliticsDocument29 pagesLESSON 1 Theories of Philippine Politicsnathaniel zNo ratings yet
- Andal Vs MacaraigDocument7 pagesAndal Vs MacaraigHoney GuideNo ratings yet
- How Capitalism Works - HowStuffWorksDocument10 pagesHow Capitalism Works - HowStuffWorksSérgio BragaNo ratings yet
- Ethical CommitteeDocument94 pagesEthical CommitteeKrupa Jyothi Perumalla100% (1)
- Slaus 210Document27 pagesSlaus 210Charitha LakmalNo ratings yet