You might also like
- Pathophysio of OsteomyelitisDocument6 pagesPathophysio of OsteomyelitisNapPeliyoNo ratings yet
- Chronic OsteomyelitisDocument35 pagesChronic OsteomyelitisMelissa Gines100% (2)
- Human Musculoskeletal System 5Sn3Document10 pagesHuman Musculoskeletal System 5Sn3Muhammad Firdauz Abdul RaisNo ratings yet
- ANATOMY of The Musculoskeletal SystemDocument3 pagesANATOMY of The Musculoskeletal Systemsigfred02No ratings yet
- Pyogenic Discitis Power PointDocument121 pagesPyogenic Discitis Power Pointjav_luv37No ratings yet
- Marrow Produce Red Blood Cells, White Blood Cells, and Platelets, A Process CalledDocument4 pagesMarrow Produce Red Blood Cells, White Blood Cells, and Platelets, A Process CalledIlyasroisulfahmiNo ratings yet
- Paper of Musculoskeletal FinishDocument23 pagesPaper of Musculoskeletal FinishHaris FernandoNo ratings yet
- Chronic OsteomyelitisDocument34 pagesChronic OsteomyelitisElenor Abrigo100% (2)
- Lec 3 Musculoskeletal SystemDocument33 pagesLec 3 Musculoskeletal SystemRavand BamerniNo ratings yet
- Muscular and Skeletal SystemDocument8 pagesMuscular and Skeletal SystemPrasad WasteNo ratings yet
- Human Anatomy 4th Edition Saladin Solutions Manual 1Document36 pagesHuman Anatomy 4th Edition Saladin Solutions Manual 1donnawugnwsjrzcxt100% (21)
- Human Anatomy 4Th Edition Saladin Solutions Manual Full Chapter PDFDocument27 pagesHuman Anatomy 4Th Edition Saladin Solutions Manual Full Chapter PDFdora.ivy892100% (16)
- Chapter IV - All About Muscles: Joint, Muscle, Tendon & LigamentDocument5 pagesChapter IV - All About Muscles: Joint, Muscle, Tendon & LigamentIndranil SinhaNo ratings yet
- The Skeleton and Muscles: Muscular & Skeletal SystemDocument2 pagesThe Skeleton and Muscles: Muscular & Skeletal SystemAbhinavNo ratings yet
- Human Anatomy 5th Edition Saladin Solutions ManualDocument7 pagesHuman Anatomy 5th Edition Saladin Solutions Manualjillhenrysetcjnzrfp100% (25)
- Presentation-Biology in Healthcare-Stage3Document31 pagesPresentation-Biology in Healthcare-Stage3alanmauriciohdzNo ratings yet
- Skeletal SYatemDocument188 pagesSkeletal SYatemJasmine GañganNo ratings yet
- Human Anatomy 5Th Edition Saladin Solutions Manual Full Chapter PDFDocument28 pagesHuman Anatomy 5Th Edition Saladin Solutions Manual Full Chapter PDFJenniferWhitebctr100% (10)
- 3-The Musculosceletal SystemDocument6 pages3-The Musculosceletal SystemEma FröhlichováNo ratings yet
- The Human Skeletal SystemDocument3 pagesThe Human Skeletal SystemFelix AyornuNo ratings yet
- Human Musculoskeletal SystemDocument11 pagesHuman Musculoskeletal SystemMuhammad NaqibNo ratings yet
- LommusculoDocument59 pagesLommusculoLibi FarrellNo ratings yet
- Types of Connective Tissue ProperDocument9 pagesTypes of Connective Tissue ProperFikri RozanNo ratings yet
- 1 Sistem MuskuloskeletalDocument27 pages1 Sistem MuskuloskeletalAshar AbilowoNo ratings yet
- Bone AnatomyDocument11 pagesBone AnatomyLiam Jacque LapuzNo ratings yet
- Introduction To The Muscular SystemDocument2 pagesIntroduction To The Muscular SystemJehannahBaratNo ratings yet
- Reviewer Zoo LecDocument27 pagesReviewer Zoo LecayeyedumpNo ratings yet
- The Skeletal SystemDocument5 pagesThe Skeletal SystemMika SaldañaNo ratings yet
- Connective TissuesDocument10 pagesConnective Tissuesbenishgulzar50No ratings yet
- 4.3 Bone TissueDocument80 pages4.3 Bone TissueManjunathNo ratings yet
- Osteomyelitis LaikaDocument4 pagesOsteomyelitis LaikaAl Lai KaNo ratings yet
- Skeletal System - mp4 - Google DriveDocument7 pagesSkeletal System - mp4 - Google Drivefaresalesa2005No ratings yet
- Week 10 (A) HSBDocument6 pagesWeek 10 (A) HSBBeyonce SkekelNo ratings yet
- Musculo Skeletal SystemDocument3 pagesMusculo Skeletal SystemMARY JOY MANALANSANNo ratings yet
- Chapter 3Document12 pagesChapter 3Deolita BadiangNo ratings yet
- BOOK1 CamilleDocument12 pagesBOOK1 CamilleSteve tarucNo ratings yet
- What Is OsteologyDocument5 pagesWhat Is Osteology69722No ratings yet
- SkeletAl SystemDocument18 pagesSkeletAl SystemYen BailadoNo ratings yet
- BonesDocument2 pagesBonesDDNo ratings yet
- Arthritic Written Report FinalDocument43 pagesArthritic Written Report FinalGlea PavillarNo ratings yet
- 7 October, 2021. Thursday Biology JointsDocument17 pages7 October, 2021. Thursday Biology JointsOyasor Ikhapo AnthonyNo ratings yet
- Osteoporosis Yang Dipengaruhi Oleh Gangguan Metabolism Dan Pembentukan TulangDocument8 pagesOsteoporosis Yang Dipengaruhi Oleh Gangguan Metabolism Dan Pembentukan TulangrioalxNo ratings yet
- Jamhuriya University of Science and Technology (JUST) : Musculoskeletal SystemDocument18 pagesJamhuriya University of Science and Technology (JUST) : Musculoskeletal SystemAnime TailNo ratings yet
- Pe Bblan AssignmentDocument2 pagesPe Bblan AssignmentOrlando Sanchez RimaNo ratings yet
- Summary of Muscosceletal System - Fuzna Dahlia M - I1J020010Document7 pagesSummary of Muscosceletal System - Fuzna Dahlia M - I1J020010Fuzna DahliaNo ratings yet
- Musculoskeletal SystemDocument7 pagesMusculoskeletal SystemKhushi JainNo ratings yet
- The Musculoskeletal System Is Composed of Two SystemsDocument3 pagesThe Musculoskeletal System Is Composed of Two SystemsKomang AyudhyaNo ratings yet
- Anatomy Psychology: "Biomechanical Movement"Document10 pagesAnatomy Psychology: "Biomechanical Movement"IlyasroisulfahmiNo ratings yet
- BiologyDocument14 pagesBiologyNur Maisarah AnuarNo ratings yet
- Human Skeletal SystemDocument25 pagesHuman Skeletal SystemEver DyNo ratings yet
- The Skeletal System HDocument23 pagesThe Skeletal System HRajorshi MishraNo ratings yet
- OrifDocument13 pagesOrifAhmabelle Mara D. AbellaNo ratings yet
- Bones and MuscleDocument3 pagesBones and MuscleRio Geline EdralinNo ratings yet
- Ana PhysioDocument6 pagesAna PhysioZyra ObedencioNo ratings yet
- Human Musculoskeletal System GotovoDocument10 pagesHuman Musculoskeletal System GotovonatalivaloNo ratings yet
- Unit 2: Bones and Cartilage Structure and Types 0F Bones and Cartilage Ossification Bone Growth and ResorptionDocument75 pagesUnit 2: Bones and Cartilage Structure and Types 0F Bones and Cartilage Ossification Bone Growth and Resorptionsourya jyoti dashNo ratings yet
- Chapter 6 Content Review Questions 1-8Document3 pagesChapter 6 Content Review Questions 1-8Rhonique MorganNo ratings yet
- Orthopaedics and Trauma for Medical Students and Junior ResidentsFrom EverandOrthopaedics and Trauma for Medical Students and Junior ResidentsRating: 5 out of 5 stars5/5 (3)
- WSD M1a283 B50Document9 pagesWSD M1a283 B50'Lampa'No ratings yet
- Bharti Airtel Strategy FinalDocument39 pagesBharti Airtel Strategy FinalniksforloveuNo ratings yet
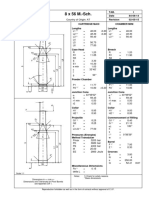
- 8 X 56 M.-SCH.: Country of Origin: ATDocument1 page8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNo ratings yet
- The Original Lists of Persons of Quality Emigrants Religious Exiles Political Rebels Serving Men Sold For A Term of Years Apprentices Children Stolen Maidens Pressed and OthersDocument609 pagesThe Original Lists of Persons of Quality Emigrants Religious Exiles Political Rebels Serving Men Sold For A Term of Years Apprentices Children Stolen Maidens Pressed and OthersShakir Daddy-Phatstacks Cannon100% (1)
- Vest3000mkii TurntableDocument16 pagesVest3000mkii TurntableElkin BabiloniaNo ratings yet
- SL Generator Ultrasunete RincoDocument2 pagesSL Generator Ultrasunete RincoDariaNo ratings yet
- Vendor Registration FormDocument4 pagesVendor Registration FormhiringNo ratings yet
- Sociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadDocument44 pagesSociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadJohn Blackburn100% (20)
- MegaMacho Drums BT READ MEDocument14 pagesMegaMacho Drums BT READ MEMirkoSashaGoggoNo ratings yet
- BAMDocument111 pagesBAMnageswara_mutyalaNo ratings yet
- Rapp 2011 TEREOS GBDocument58 pagesRapp 2011 TEREOS GBNeda PazaninNo ratings yet
- Introduction Spreadable Media TtsDocument22 pagesIntroduction Spreadable Media TtsYanro FerrerNo ratings yet
- HR Practices in Public Sector Organisations: (A Study On APDDCF LTD.)Document28 pagesHR Practices in Public Sector Organisations: (A Study On APDDCF LTD.)praffulNo ratings yet
- DBM Uv W ChartDocument2 pagesDBM Uv W ChartEddie FastNo ratings yet
- Intro To MavenDocument18 pagesIntro To MavenDaniel ReckerthNo ratings yet
- Army Aviation Digest - Apr 1971Document68 pagesArmy Aviation Digest - Apr 1971Aviation/Space History LibraryNo ratings yet
- 4039-Texto Del Artículo-12948-3-10-20211123Document14 pages4039-Texto Del Artículo-12948-3-10-20211123Ricardo ApazaNo ratings yet
- Addendum ESIA Oct 2019Document246 pagesAddendum ESIA Oct 2019melkamuNo ratings yet
- Current Harmonics: Electric Power System Power QualityDocument3 pagesCurrent Harmonics: Electric Power System Power QualityAlliver SapitulaNo ratings yet
- FIREBASE Edited PresentationDocument12 pagesFIREBASE Edited PresentationNiraj MirgalNo ratings yet
- Vanguard 44 - Anti Tank Helicopters PDFDocument48 pagesVanguard 44 - Anti Tank Helicopters PDFsoljenitsin250% (2)
- 15 Miscellaneous Bacteria PDFDocument2 pages15 Miscellaneous Bacteria PDFAnne MorenoNo ratings yet
- Thermodynamics WorksheetDocument5 pagesThermodynamics WorksheetMalcolmJustMalcolmNo ratings yet
- Springs: All India Distributer of NienhuisDocument35 pagesSprings: All India Distributer of NienhuisIrina DroliaNo ratings yet
- Exclusive GA MCQs For IBPS Clerk MainDocument136 pagesExclusive GA MCQs For IBPS Clerk MainAnkit MauryaNo ratings yet
- E Voting PPT - 1Document11 pagesE Voting PPT - 1madhu100% (2)
- Work Sample 2 - Eoc and CrucibleDocument35 pagesWork Sample 2 - Eoc and Crucibleapi-259791703No ratings yet
- Nat Steel BREGENEPD000379Document16 pagesNat Steel BREGENEPD000379Batu GajahNo ratings yet
- ARIIX - Clean - Eating - Easy - Ecipes - For - A - Healthy - Life - Narx PDFDocument48 pagesARIIX - Clean - Eating - Easy - Ecipes - For - A - Healthy - Life - Narx PDFAnte BaškovićNo ratings yet
- Study Notes - Google Project Management Professional CertificateDocument4 pagesStudy Notes - Google Project Management Professional CertificateSWAPNIL100% (1)