You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Indications and Complications of ErcpDocument57 pagesIndications and Complications of ErcpNuha AL-YousfiNo ratings yet
- Doctors Without BordersDocument10 pagesDoctors Without Bordersapi-396919069No ratings yet
- Elisa Product ListDocument18 pagesElisa Product ListVinsmoke SanjiNo ratings yet
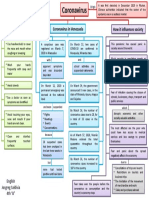
- Mapa Mental Coronavirus en InglesDocument1 pageMapa Mental Coronavirus en InglestavimayrNo ratings yet
- Lockdown Leaves Private Hostel OwnersDocument6 pagesLockdown Leaves Private Hostel OwnersamatyaadibeshNo ratings yet
- Insecticide Resistance To Anopheles Spp. Mosquitoes (Diptera: Culicidae) in Nigeria: A ReviewDocument9 pagesInsecticide Resistance To Anopheles Spp. Mosquitoes (Diptera: Culicidae) in Nigeria: A ReviewYusuf UmarNo ratings yet
- Case Control Study Design: Ni Luh Putu Ariastuti, MD., MPHDocument26 pagesCase Control Study Design: Ni Luh Putu Ariastuti, MD., MPHtrimayunikaNo ratings yet
- Alkaline HydrolysisDocument28 pagesAlkaline Hydrolysissiamak77No ratings yet
- Emerging and Re Emerging Disease Community Healty NursingDocument38 pagesEmerging and Re Emerging Disease Community Healty Nursinghemihema100% (2)
- Body Mass Index (BMI)Document13 pagesBody Mass Index (BMI)RamsrajNo ratings yet
- Low Back PainDocument80 pagesLow Back PainJagdish AgroyaNo ratings yet
- Kirit P. Mehta School of Law, Mumbai: A Project Submitted ONDocument12 pagesKirit P. Mehta School of Law, Mumbai: A Project Submitted ONNikit BaryaNo ratings yet
- COVID-19 Outbreak in Malaysia: Actions Taken by The Malaysian GovernmentDocument32 pagesCOVID-19 Outbreak in Malaysia: Actions Taken by The Malaysian GovernmentIrfan AzaharNo ratings yet
- Endodontics DiagnosisDocument6 pagesEndodontics DiagnosisRPNo ratings yet
- EntomologistDocument4 pagesEntomologistapi-79028662No ratings yet
- Fitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDocument30 pagesFitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDellNo ratings yet
- Nursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationPaul Cubacub100% (1)
- Furuncle and Carbuncle FootDocument0 pagesFuruncle and Carbuncle Footrasputin22100% (1)
- Bijnor Thesis Research by Pragya SrivastavaDocument291 pagesBijnor Thesis Research by Pragya SrivastavaPragya Srivastava AgrawalNo ratings yet
- A Case of Lateral Rectus Palsy by DR Sunil KannadaDocument5 pagesA Case of Lateral Rectus Palsy by DR Sunil KannadaHomoeopathic Pulse100% (1)
- The Cariogram Indicates A High Risk For CariesDocument3 pagesThe Cariogram Indicates A High Risk For CariesDyahAyuRisqiNilamsariNo ratings yet
- Deaths From COVID-19 in Healthcare Workers in Italy - What Can We Learn?Document2 pagesDeaths From COVID-19 in Healthcare Workers in Italy - What Can We Learn?Dimitri MandolesiNo ratings yet
- Multiple Choice QuestionsDocument5 pagesMultiple Choice QuestionsDr Sumant Sharma80% (10)
- Essay-Mike Lemuel BacayoDocument1 pageEssay-Mike Lemuel BacayoLem MikeeNo ratings yet
- Review Oral Pathology PDFDocument3 pagesReview Oral Pathology PDFpuipuiii100% (1)
- TISS Sample Paper - MA in Public Health in Social Epidemiology Part 2Document12 pagesTISS Sample Paper - MA in Public Health in Social Epidemiology Part 2bhustlero0oNo ratings yet
- Fever With Rash in Table Form.Document4 pagesFever With Rash in Table Form.Azizan HannyNo ratings yet
- Reflection - Sonny Boy A. Sajonia - Bsba 1BDocument2 pagesReflection - Sonny Boy A. Sajonia - Bsba 1BSonny Boy SajoniaNo ratings yet
- Vesicoureteral Reflux: Done By: Khalid Al-Qudsi Faisal Burghal Supervised By: Dr. Osama Bani HaniDocument27 pagesVesicoureteral Reflux: Done By: Khalid Al-Qudsi Faisal Burghal Supervised By: Dr. Osama Bani HaniRashed ShatnawiNo ratings yet
- Adverse Drug ReactionDocument15 pagesAdverse Drug ReactionPuji Arifianti RamadhanyNo ratings yet