You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Ageloc Lumispa: Out of StockDocument1 pageAgeloc Lumispa: Out of StockMaria LpzNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Differences in SinsDocument3 pagesThe Differences in SinsMaria LpzNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Excel Bill of Quantities SampleDocument15 pagesExcel Bill of Quantities SampleMaria LpzNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Karwa Driving School Expansion General SummaryDocument2 pagesKarwa Driving School Expansion General SummaryMaria LpzNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Huawei Watch User Guide 01 EnglishDocument62 pagesHuawei Watch User Guide 01 EnglishAkrama HussainNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Nurses, Negligence, Malpractice: An Analysis Based On More Than 250 Cases Against NursesDocument10 pagesNurses, Negligence, Malpractice: An Analysis Based On More Than 250 Cases Against NursesLesterNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
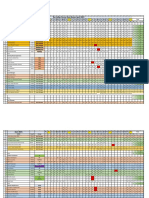
- Ras Laffan Nurses Duty Roster April-2021 April 2021Document3 pagesRas Laffan Nurses Duty Roster April-2021 April 2021Maria LpzNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Sacrament of ReconciliationDocument11 pagesThe Sacrament of ReconciliationMaria LpzNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Divine Mercy Novena 2021 - M1Document85 pagesDivine Mercy Novena 2021 - M1Maria LpzNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Bill No. 2 - Office BuildingDocument28 pagesBill No. 2 - Office BuildingMaria LpzNo ratings yet
- Bill No. 4 - Generator RoomDocument13 pagesBill No. 4 - Generator RoomMaria LpzNo ratings yet
- Bill No. 1 - PreliminariesDocument20 pagesBill No. 1 - PreliminariesMaria LpzNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- PROGRAMDocument1 pagePROGRAMMaria LpzNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nurses, Negligence, Malpractice: An Analysis Based On More Than 250 Cases Against NursesDocument10 pagesNurses, Negligence, Malpractice: An Analysis Based On More Than 250 Cases Against NursesLesterNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Drug Dosage and IV Rates Calculations PDFDocument6 pagesDrug Dosage and IV Rates Calculations PDFvarmaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- US4Document4 pagesUS4Maria LpzNo ratings yet
- Drug Dosage and IV Rates Calculations PDFDocument6 pagesDrug Dosage and IV Rates Calculations PDFvarmaNo ratings yet
- Paediatric Nursing: Faculty of Engineering, Health, Science & Theenvironment/School of HealthDocument2 pagesPaediatric Nursing: Faculty of Engineering, Health, Science & Theenvironment/School of HealthMaria LpzNo ratings yet
- UNIV 205 Whistleblowing Case Study: Nusayba Abdelmagid Maria Baluya Amira NajiDocument16 pagesUNIV 205 Whistleblowing Case Study: Nusayba Abdelmagid Maria Baluya Amira NajiMaria LpzNo ratings yet
- Experience in GhanaDocument12 pagesExperience in GhanaMaria LpzNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Care PlanDocument2 pagesNursing Care PlanMaria LpzNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Reflective AssignmentDocument5 pagesReflective AssignmentVictor Murambiwa100% (3)
- Nursing Family Community Wellness Diagnoses SuttonDocument6 pagesNursing Family Community Wellness Diagnoses SuttonMaria LpzNo ratings yet
- Ref 4 FinDocument1 pageRef 4 FinMaria LpzNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Nursing Care PlanDocument12 pagesNursing Care Planzsazsageorge86% (21)
- Transfer and Edit ImagesDocument5 pagesTransfer and Edit ImagesMaria LpzNo ratings yet
- Effectiveness of Hourly RoundingDocument7 pagesEffectiveness of Hourly RoundingMaria Lpz100% (1)
- Nursing Family Community Wellness Diagnoses SuttonDocument6 pagesNursing Family Community Wellness Diagnoses SuttonMaria LpzNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Daftar PustakaDocument3 pagesDaftar PustakaAdnanNo ratings yet
- Colon 2014597 D FHTDocument4 pagesColon 2014597 D FHTyoohooNo ratings yet
- Lesson 7 - Organ TransplantationDocument14 pagesLesson 7 - Organ TransplantationJosee100% (1)
- The "Five Families" College Essay ExampleDocument1 pageThe "Five Families" College Essay ExampleKishor RaiNo ratings yet
- Nervous Responses of EarthwormDocument27 pagesNervous Responses of EarthwormKayla JoezetteNo ratings yet
- 4546-LacOperon InstsDocument14 pages4546-LacOperon InstsScribd_is_GreatNo ratings yet
- Young Children's Biological Predisposition To Learn in Privileged DomainDocument6 pagesYoung Children's Biological Predisposition To Learn in Privileged DomainVeronica Dadal0% (1)
- C. S. Sureka, Christina Armpilia - Radiation Biology For Medical Physicists (2017, CRC Press, Taylor & Francis Group) - 148-163Document16 pagesC. S. Sureka, Christina Armpilia - Radiation Biology For Medical Physicists (2017, CRC Press, Taylor & Francis Group) - 148-163dwi riris indriyaniNo ratings yet
- (PDF) Root Growth of Phalsa (Grewia Asiatica L.) As Affected by Type of CuttDocument5 pages(PDF) Root Growth of Phalsa (Grewia Asiatica L.) As Affected by Type of CuttAliNo ratings yet
- DNA Replication Practice PDFDocument2 pagesDNA Replication Practice PDFKim100% (1)
- Komiyama Et Al., (2008) Allometry, Biomass, and Productivity of Mangrove Forests A ReviewDocument11 pagesKomiyama Et Al., (2008) Allometry, Biomass, and Productivity of Mangrove Forests A ReviewVandhi Amali100% (1)
- Biofuels Bioprod Bioref - 2022 - Souza - Bioenergy Research in Brazil A Bibliometric Evaluation of The BIOEN ResearchDocument16 pagesBiofuels Bioprod Bioref - 2022 - Souza - Bioenergy Research in Brazil A Bibliometric Evaluation of The BIOEN Researchdeborah151No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Plant Transport - IGCSE Biology Notes (2020)Document6 pagesPlant Transport - IGCSE Biology Notes (2020)Zhi En LeeNo ratings yet
- Week 6. Definision and DictionaryDocument19 pagesWeek 6. Definision and DictionaryafdreliautariazizahNo ratings yet
- 8 Cell - The Unit of Life-NotesDocument6 pages8 Cell - The Unit of Life-NotesBhavanya RavichandrenNo ratings yet
- Organizing A TextDocument3 pagesOrganizing A TextMercedes Jimenez RomanNo ratings yet
- Chapter 2 Medical Terminology Verified AnswersDocument5 pagesChapter 2 Medical Terminology Verified AnswersGregg ProducerNo ratings yet
- Protochordata FIXDocument33 pagesProtochordata FIXSylvia AnggraeniNo ratings yet
- Starship Troopers Skinnies Army BookDocument66 pagesStarship Troopers Skinnies Army BookDougBirtles100% (5)
- Essay On Physical SelfDocument2 pagesEssay On Physical Selfcmestrada03No ratings yet
- Geology of Malta and GozoDocument6 pagesGeology of Malta and GozoCarolina Pérez P.No ratings yet
- UAS Writing For Discourse - 4 Pagi OkDocument1 pageUAS Writing For Discourse - 4 Pagi Oksalwa syabinaNo ratings yet
- Ficha Técnica SpotcheckDocument5 pagesFicha Técnica SpotcheckJuan PazNo ratings yet
- Artigo Sobre Nutrigenômica e Nutrigenética PDFDocument18 pagesArtigo Sobre Nutrigenômica e Nutrigenética PDFDiogo JuniorNo ratings yet
- 02 Anatomy and Histology PLE 2019 RatioDocument69 pages02 Anatomy and Histology PLE 2019 RatioPatricia VillegasNo ratings yet
- Crop Sci 1 Lecture Manual OverviewDocument86 pagesCrop Sci 1 Lecture Manual OverviewAnalYn Litawan Bucasan100% (1)
- Natamycin Story - What You Need to KnowDocument13 pagesNatamycin Story - What You Need to KnowCharles MardiniNo ratings yet
- Module 2 NCM 114Document11 pagesModule 2 NCM 114Erven AranasNo ratings yet
- Molecular Genetics of Colorectal Cancer - UpToDateDocument41 pagesMolecular Genetics of Colorectal Cancer - UpToDateToweran ToweraneNo ratings yet
- Chapter 5Document14 pagesChapter 5Caitlin G.No ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)