You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Dolor y Fatiga en El Deporte Son Tan Diferentes PDFDocument3 pagesDolor y Fatiga en El Deporte Son Tan Diferentes PDFRamiro Tabilo MaluendaNo ratings yet
- Strutt - 2008 - Manual-Therapy - Patients Perceptions and Satisfaction With Treatment in A UK PDFDocument12 pagesStrutt - 2008 - Manual-Therapy - Patients Perceptions and Satisfaction With Treatment in A UK PDFRamiro Tabilo MaluendaNo ratings yet
- El Efecto de La Educación en Neurociencia Sobre El Dolor, La Discapacidad, La Ansiedad y El Estrés en El Dolor Musculoesquelético Crónico PDFDocument16 pagesEl Efecto de La Educación en Neurociencia Sobre El Dolor, La Discapacidad, La Ansiedad y El Estrés en El Dolor Musculoesquelético Crónico PDFRamiro Tabilo MaluendaNo ratings yet
- Efecto de Los Ejercicios de Control Motor Frente A La Actividad Gradual en Pacientes Con Dolor Lumbar Inespecífico Crónico Un Ensayo Controlado Aleatorizado PDFDocument18 pagesEfecto de Los Ejercicios de Control Motor Frente A La Actividad Gradual en Pacientes Con Dolor Lumbar Inespecífico Crónico Un Ensayo Controlado Aleatorizado PDFRamiro Tabilo MaluendaNo ratings yet
- Schmid 2008 Manual-Therapy PDFDocument10 pagesSchmid 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Kaale 2008 Manual-Therapy PDFDocument7 pagesKaale 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Entrenamiento Propioceptivo PDFDocument179 pagesEntrenamiento Propioceptivo PDFRamiro Tabilo MaluendaNo ratings yet
- El Poder de La Educación Sobre El Dolor Un Llamado para Una Investigación Sólida PDFDocument1 pageEl Poder de La Educación Sobre El Dolor Un Llamado para Una Investigación Sólida PDFRamiro Tabilo MaluendaNo ratings yet
- Actividad Muscular Escapular en Una Variedad de Ejercicios Pliométricos.Document28 pagesActividad Muscular Escapular en Una Variedad de Ejercicios Pliométricos.Ramiro Tabilo MaluendaNo ratings yet
- (First Author) 2008 Manual-Therapy 1 PDFDocument1 page(First Author) 2008 Manual-Therapy 1 PDFRamiro Tabilo MaluendaNo ratings yet
- Anatomy Trains PDFDocument3 pagesAnatomy Trains PDFRamiro Tabilo Maluenda100% (1)
- Nuevo Documento de TextoDocument1 pageNuevo Documento de TextoRamiro Tabilo MaluendaNo ratings yet
- Effects of Low-Intensity Cycle Training With Restricted Leg Blood Flow On Thigh Muscle Volume and VO2MAX in Young MenDocument7 pagesEffects of Low-Intensity Cycle Training With Restricted Leg Blood Flow On Thigh Muscle Volume and VO2MAX in Young MenRamiro Tabilo MaluendaNo ratings yet
- Actividad Muscular Escapular en Una Variedad de Ejercicios Pliométricos.Document28 pagesActividad Muscular Escapular en Una Variedad de Ejercicios Pliométricos.Ramiro Tabilo MaluendaNo ratings yet
- (First Author) 2008 Manual-Therapy PDFDocument1 page(First Author) 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Tartaglia - 2008 - Manual-Therapy - Masticatory Muscle Activity During Maximum Voluntary Clench in PDFDocument7 pagesTartaglia - 2008 - Manual-Therapy - Masticatory Muscle Activity During Maximum Voluntary Clench in PDFRamiro Tabilo MaluendaNo ratings yet
- Feleus 2008 Manual-Therapy PDFDocument8 pagesFeleus 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Grewar 2008 Manual-Therapy PDFDocument12 pagesGrewar 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Lee 2008 Manual-Therapy PDFDocument7 pagesLee 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Casserley-Feeney 2008 Manual-Therapy PDFDocument9 pagesCasserley-Feeney 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Ocarino 2008 Manual-Therapy PDFDocument8 pagesOcarino 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Murphy 2008 Manual-Therapy PDFDocument5 pagesMurphy 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Assink 2008 Manual-Therapy PDFDocument6 pagesAssink 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- Beeton 2008 Manual-Therapy PDFDocument2 pagesBeeton 2008 Manual-Therapy PDFRamiro Tabilo MaluendaNo ratings yet
- A Guide To Physical Therapist Practice. Volume I PDFDocument58 pagesA Guide To Physical Therapist Practice. Volume I PDFRamiro Tabilo Maluenda100% (1)
- El Modelo Continuo de La Patología Tendinosa Cuál Es Su Mérito en La Práctica Clínica y La InvestigaciónDocument8 pagesEl Modelo Continuo de La Patología Tendinosa Cuál Es Su Mérito en La Práctica Clínica y La InvestigaciónRamiro Tabilo MaluendaNo ratings yet
- Dry Needling - Spinal Cord Mechanism PDFDocument8 pagesDry Needling - Spinal Cord Mechanism PDFRamiro Tabilo MaluendaNo ratings yet
- PainDocument7 pagesPainocoxodoNo ratings yet
- Dry Needling - Techniques Outcomes PDFDocument6 pagesDry Needling - Techniques Outcomes PDFRamiro Tabilo MaluendaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PRI Integ For Pediatrics (Nov 2020) - Complete ManualDocument208 pagesPRI Integ For Pediatrics (Nov 2020) - Complete Manualzhang yangNo ratings yet
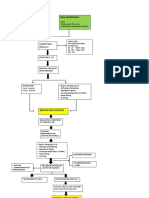
- RDS PathophysiologyDocument2 pagesRDS PathophysiologyADATO, Alaiza Mae S.No ratings yet
- Physiotherapy in Respiratory Care 3rd Ed - A. Hough (Nelson Thornes, 2001) WW PDFDocument562 pagesPhysiotherapy in Respiratory Care 3rd Ed - A. Hough (Nelson Thornes, 2001) WW PDFDaria Nectaria100% (1)
- Science Class 8 Respiration and CirculationDocument9 pagesScience Class 8 Respiration and Circulationamnakazmi100% (1)
- Burn 160909021524Document30 pagesBurn 160909021524vivek100% (1)
- SMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Document16 pagesSMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Azie HarunNo ratings yet
- Kindergarten: Quarter 1: Week 4 Learning ExperiencesDocument24 pagesKindergarten: Quarter 1: Week 4 Learning ExperiencesHanzel NietesNo ratings yet
- R E G U L A T I O N S: JohannesburgDocument24 pagesR E G U L A T I O N S: JohannesburgdchunNo ratings yet
- Bio Circulation Sba SumnDocument6 pagesBio Circulation Sba SumnNelicia WilliamsNo ratings yet
- Yoga PosesDocument29 pagesYoga PosesthippliNo ratings yet
- OB. CH 14 Study GuideDocument5 pagesOB. CH 14 Study GuidePaige Nicole GauthreauxNo ratings yet
- Neonatal Ventilation - Basics of Mechanical Ventilation: Authors: Sam Wallis - Catriona FirthDocument21 pagesNeonatal Ventilation - Basics of Mechanical Ventilation: Authors: Sam Wallis - Catriona FirthEduardo Rios DuboisNo ratings yet
- Yoga For Eyes: Improve Eyesight NaturallyDocument14 pagesYoga For Eyes: Improve Eyesight NaturallyAshish GadnayakNo ratings yet
- Experiment On Cellular Respiration (Using BTB Solution)Document4 pagesExperiment On Cellular Respiration (Using BTB Solution)Lorraine M. Del RosarioNo ratings yet
- School of The Prophets by Larent and Stewart, 1922Document53 pagesSchool of The Prophets by Larent and Stewart, 1922sirjsslut100% (1)
- Evita v800 v600 SW 1n Ifu 9055601 en PDFDocument336 pagesEvita v800 v600 SW 1n Ifu 9055601 en PDFNandhini SivakumarNo ratings yet
- NCM 109 Common Health Problems in TodddlersDocument9 pagesNCM 109 Common Health Problems in TodddlersMantilla, Kristina Cassandra A.No ratings yet
- Interoceptive Rhythms in The BrainDocument15 pagesInteroceptive Rhythms in The BrainAlisson Araya HNo ratings yet
- ALEX MICA Lyrics - For MergeDocument2 pagesALEX MICA Lyrics - For MergeHyuga Tiger HmNo ratings yet
- MiofuncionalDocument9 pagesMiofuncionalKaterine TrillosNo ratings yet
- DumoDocument3 pagesDumoWangshosanNo ratings yet
- Jake YAN - Ib - Biology - Key - Practicals - Revision - TaskDocument10 pagesJake YAN - Ib - Biology - Key - Practicals - Revision - TaskJake YANNo ratings yet
- Physiology Magdy Sabry RespiratoryDocument100 pagesPhysiology Magdy Sabry Respiratoryإبراهيم عسيري100% (3)
- Unit 4Document77 pagesUnit 420BM002 AKSHAYANo ratings yet
- Advantage 1000 Full-Facepiece Respirator Instruction Manual - EN PDFDocument12 pagesAdvantage 1000 Full-Facepiece Respirator Instruction Manual - EN PDFHồng Thái Nguyễn MicroBiologyNo ratings yet
- PrehospitalCTASParamedicGuide December312016 Version2.0 PDFDocument98 pagesPrehospitalCTASParamedicGuide December312016 Version2.0 PDFSaifullah RachmanNo ratings yet
- Cambridge Secondary 1 CheckpointDocument20 pagesCambridge Secondary 1 CheckpointAnisahNo ratings yet
- Transient Tachypnea of The NewbornDocument2 pagesTransient Tachypnea of The Newbornjulesubayubay5428No ratings yet
- 7-Day Arm WorkoutDocument8 pages7-Day Arm WorkoutHarshit Singh100% (1)
- DLP in HealthDocument7 pagesDLP in HealthrodalynbagcalNo ratings yet