You might also like
- My Testament On The Fabiana Arejola M...Document17 pagesMy Testament On The Fabiana Arejola M...Jaime G. Arejola100% (1)
- North American Indians - A Very Short IntroductionDocument147 pagesNorth American Indians - A Very Short IntroductionsiesmannNo ratings yet
- Ashforth & Mael 1989 Social Identity Theory and The OrganizationDocument21 pagesAshforth & Mael 1989 Social Identity Theory and The Organizationhoorie100% (1)
- GIT Problems GuideDocument70 pagesGIT Problems GuidetantanbaragoNo ratings yet
- Assessing The AbdomenDocument82 pagesAssessing The AbdomenHyacinth Jane Dela PeñaNo ratings yet
- NCM 116 GEP MIDTERMDocument20 pagesNCM 116 GEP MIDTERMKM PanganibanNo ratings yet
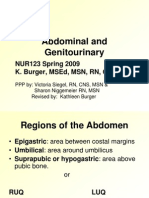
- WEB Abdominal and GenitourinaryDocument31 pagesWEB Abdominal and GenitourinaryJack MiguelNo ratings yet
- Unit Vii Assessment of The Abdomen, Anus and RectumDocument86 pagesUnit Vii Assessment of The Abdomen, Anus and Rectumramzan aliNo ratings yet
- Chronic DiarrheaDocument38 pagesChronic DiarrheaShujina ZainabNo ratings yet
- Nursing Assessment: Gastrointestinal System: Tuti SeniwatiDocument42 pagesNursing Assessment: Gastrointestinal System: Tuti SeniwatiSlamet KatibNo ratings yet
- Bowel EliminationDocument67 pagesBowel EliminationPhyu Lin100% (1)
- D. G.IDocument23 pagesD. G.IGloryJane100% (1)
- Intestinal ObstructionDocument27 pagesIntestinal ObstructionAna AvilaNo ratings yet
- Chronic DiarrheaDocument66 pagesChronic DiarrheaJulita Yanti100% (1)
- Bowel EliminationDocument66 pagesBowel EliminationIvAn Cordova CruzNo ratings yet
- Git DisturbancesDocument119 pagesGit DisturbancesPeterpan NguyenNo ratings yet
- Chole EndorseDocument52 pagesChole EndorseSimon Peter MollanedaNo ratings yet
- Introduction to Digestive System DisordersDocument7 pagesIntroduction to Digestive System DisordersAloshNo ratings yet
- L 9. Physiology & Disorders of StomachDocument52 pagesL 9. Physiology & Disorders of Stomachsjfk1416No ratings yet
- CA Stomach 1Document23 pagesCA Stomach 1Ticky TomNo ratings yet
- Day 7 Peptic-Ulcer-AppendicitisDocument27 pagesDay 7 Peptic-Ulcer-AppendicitisTrisha UmaliNo ratings yet
- Metab II DiverticulosisDocument94 pagesMetab II DiverticulosisEthel Lourdes Cornejo AmodiaNo ratings yet
- Funda 2Document59 pagesFunda 2nucahersheyskatNo ratings yet
- Abdominal anatomy assessment: Key techniques for inspection, auscultation, percussion and palpationDocument55 pagesAbdominal anatomy assessment: Key techniques for inspection, auscultation, percussion and palpationJackie BringhurstNo ratings yet
- Acute AbdomenDocument53 pagesAcute AbdomenMahdi DiabNo ratings yet
- Pengkajian Sistem PencernaanDocument44 pagesPengkajian Sistem Pencernaanmusa_nindaNo ratings yet
- Digestive SystemDocument13 pagesDigestive SystemIndah Maharani NasutionNo ratings yet
- History and Examination: GIT System: Ahmed Laving Paediatric GastroenterologistDocument27 pagesHistory and Examination: GIT System: Ahmed Laving Paediatric Gastroenterologistokwadha simionNo ratings yet
- Presented By:: Alia - Farooq & Zahra - AbbasDocument43 pagesPresented By:: Alia - Farooq & Zahra - AbbasZahra MotorwalaNo ratings yet
- Guide to History Taking and Examination of Patients with Abdominal DisordersDocument46 pagesGuide to History Taking and Examination of Patients with Abdominal Disordersخديجة عمرNo ratings yet
- Digestive SystemDocument65 pagesDigestive SystemRuel AlejandroNo ratings yet
- Lecture 4 - Spasmodic Colic HorseDocument20 pagesLecture 4 - Spasmodic Colic HorseUNICORN TIMENo ratings yet
- PERITONITISDocument12 pagesPERITONITISHayat AL AKOUM100% (1)
- Gastrointestinal and HepatobiliaryDocument54 pagesGastrointestinal and Hepatobiliaryjeshema100% (1)
- Gastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcDocument67 pagesGastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcMuath AlzghlellatNo ratings yet
- Medical Surgical Nursing The Gastro-Intestinal System Nurse Licensure Examination Review By: John Mark B. Pocsidio, RN, Usrn, MSNDocument22 pagesMedical Surgical Nursing The Gastro-Intestinal System Nurse Licensure Examination Review By: John Mark B. Pocsidio, RN, Usrn, MSNjm_pocsidio8213No ratings yet
- Elimination PatternDocument50 pagesElimination Patternmamoonazafar2No ratings yet
- Ferret Medicine and Surgery: Dr. Szabó ZoltánDocument121 pagesFerret Medicine and Surgery: Dr. Szabó ZoltánaaarrrqazNo ratings yet
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 pagesPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedNo ratings yet
- 1 Approach To DiarrheaDocument37 pages1 Approach To DiarrheamusabNo ratings yet
- Bowel ObstructionDocument48 pagesBowel ObstructionPatrick John100% (1)
- Nursing Stomach NotesDocument5 pagesNursing Stomach Noteslucas dibenedettoNo ratings yet
- Enterectomy (Resection For Congenital Atresia)Document4 pagesEnterectomy (Resection For Congenital Atresia)drnareshkumar3281No ratings yet
- Abd. Urinary 1Document39 pagesAbd. Urinary 1emir krlpNo ratings yet
- Abdominal SonographyDocument6 pagesAbdominal SonographyRio FutabaNo ratings yet
- Bowel Elimination Chapter SummaryDocument33 pagesBowel Elimination Chapter SummaryMaurice Ann MarquezNo ratings yet
- Pengayaan Gastro 1 - KonsepDocument43 pagesPengayaan Gastro 1 - KonsepRamaNo ratings yet
- S13 Penyakit Dan Kelainan Sistem Gastrointestinal Dan Pankreatobilier Di Bidang BedahDocument143 pagesS13 Penyakit Dan Kelainan Sistem Gastrointestinal Dan Pankreatobilier Di Bidang BedahDjamnur AgnessiaNo ratings yet
- An Unusual Case of Midgut VolvulusDocument31 pagesAn Unusual Case of Midgut VolvulusJavaid KhanNo ratings yet
- Acute Pancreatitis My LectureDocument57 pagesAcute Pancreatitis My LectureAli Nawaz khanNo ratings yet
- Student Copy of Gastrointestinal Problems SP 2010 IggyDocument80 pagesStudent Copy of Gastrointestinal Problems SP 2010 IggyJade CentinoNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Gastrointestinal Bleeding Causes, Symptoms and TreatmentDocument84 pagesGastrointestinal Bleeding Causes, Symptoms and TreatmentAngela Kristiana IntanNo ratings yet
- GIS лекция №2 синдр желуд дисп 2015 - копия - копияDocument85 pagesGIS лекция №2 синдр желуд дисп 2015 - копия - копияvelumurikavyaNo ratings yet
- FPE Gastroenterology Exam ReviewDocument55 pagesFPE Gastroenterology Exam ReviewRawda IbrahimNo ratings yet
- Medicine Case Discussion: - Roll No - 202 - 205 - 208Document30 pagesMedicine Case Discussion: - Roll No - 202 - 205 - 208Anagha M NairNo ratings yet
- Gastrointestinal DiseasesDocument19 pagesGastrointestinal DiseasesJune DumdumayaNo ratings yet
- Clinical Approach To Abdominal Disorder: Kurniyanto Department of Internal MedicineDocument68 pagesClinical Approach To Abdominal Disorder: Kurniyanto Department of Internal MedicineMonica AnggiNo ratings yet
- My Gi Lec...Document34 pagesMy Gi Lec...michelleduran72No ratings yet
- Pedia PPT1Document52 pagesPedia PPT1Jan Mikhail FrascoNo ratings yet
- Genito-Urinary Tract Disorders By: Mtespiriturnmd: NephronDocument10 pagesGenito-Urinary Tract Disorders By: Mtespiriturnmd: NephronCristybaby MunozNo ratings yet
- Jaimini Astrology - Calculation of Mandook Dasha With A Case StudyDocument6 pagesJaimini Astrology - Calculation of Mandook Dasha With A Case StudyANTHONY WRITER100% (3)
- Experiment 5 ADHAVANDocument29 pagesExperiment 5 ADHAVANManoj Raj RajNo ratings yet
- Subarachnoid Cisterns & Cerebrospinal FluidDocument41 pagesSubarachnoid Cisterns & Cerebrospinal Fluidharjoth395No ratings yet
- Republic v. EncelanDocument2 pagesRepublic v. EncelanKyla ReyesNo ratings yet
- Grecian Urn PaperDocument2 pagesGrecian Urn PaperrhesajanubasNo ratings yet
- New Manual of Fiber Science Revised (Tet)Document43 pagesNew Manual of Fiber Science Revised (Tet)RAZA Khn100% (1)
- Book of ProtectionDocument69 pagesBook of ProtectiontrungdaongoNo ratings yet
- Assignment Chemical Bonding JH Sir-4163 PDFDocument70 pagesAssignment Chemical Bonding JH Sir-4163 PDFAkhilesh AgrawalNo ratings yet
- Pengaruh Implementasi Sistem Irigasi Big Gun Sprinkler Dan Bahan Organik Terhadap Kelengasan Tanah Dan Produksi Jagung Di Lahan KeringDocument10 pagesPengaruh Implementasi Sistem Irigasi Big Gun Sprinkler Dan Bahan Organik Terhadap Kelengasan Tanah Dan Produksi Jagung Di Lahan KeringDonny Nugroho KalbuadiNo ratings yet
- Budokon - Mma.program 2012 13Document10 pagesBudokon - Mma.program 2012 13Emilio DiazNo ratings yet
- Day1 1Document17 pagesDay1 1kaganp784No ratings yet
- Engb546 NP RevisedDocument5 pagesEngb546 NP RevisedRafaelaNo ratings yet
- Veerabhadra Swamy MantrasDocument6 pagesVeerabhadra Swamy Mantrasगणेश पराजुलीNo ratings yet
- Asian Paints Research ProposalDocument1 pageAsian Paints Research ProposalYASH JOHRI-DM 21DM222No ratings yet
- Us Aers Roadmap Noncontrolling Interest 2019 PDFDocument194 pagesUs Aers Roadmap Noncontrolling Interest 2019 PDFUlii PntNo ratings yet
- Forum On Special Educational Needs: Phil Dexter Sharon Noseley Sophie FaragDocument14 pagesForum On Special Educational Needs: Phil Dexter Sharon Noseley Sophie Faragelena biancaNo ratings yet
- 2009 IBP ElectionsDocument77 pages2009 IBP ElectionsBaldovino VenturesNo ratings yet
- Critters Table MannersDocument3 pagesCritters Table Mannersapi-248006371No ratings yet
- Rak Single DentureDocument48 pagesRak Single Denturerakes0No ratings yet
- Case Problems For Management ScienceDocument11 pagesCase Problems For Management ScienceMargarita AtanacioNo ratings yet
- Importance of SimilesDocument10 pagesImportance of Similesnabeelajaved0% (1)
- Grammar activities and exercisesDocument29 pagesGrammar activities and exercisesElena NicolauNo ratings yet
- De Broglie's Hypothesis: Wave-Particle DualityDocument4 pagesDe Broglie's Hypothesis: Wave-Particle DualityAvinash Singh PatelNo ratings yet
- mc1776 - Datasheet PDFDocument12 pagesmc1776 - Datasheet PDFLg GnilNo ratings yet
- Elderly Suicide FactsDocument2 pagesElderly Suicide FactsThe News-HeraldNo ratings yet
- Radical Acceptance Guided Meditations by Tara Brach PDFDocument3 pagesRadical Acceptance Guided Meditations by Tara Brach PDFQuzzaq SebaNo ratings yet
- Contribution Sushruta AnatomyDocument5 pagesContribution Sushruta AnatomyEmmanuelle Soni-DessaigneNo ratings yet