You might also like
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Occlusion, Malocclusion and Method of Measurements - An OverviewDocument7 pagesOcclusion, Malocclusion and Method of Measurements - An OverviewDiana BernardNo ratings yet
- Dental Occlusion Past Present Future Turp Greene Strub J Oral Rehab 2008Document8 pagesDental Occlusion Past Present Future Turp Greene Strub J Oral Rehab 2008Ankita JhalaniNo ratings yet
- Philosophy of OcclusionDocument23 pagesPhilosophy of OcclusionAnil SukumaranNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Clinical Evaluation of Abutment Teeth of Removable PartialDocument7 pagesClinical Evaluation of Abutment Teeth of Removable PartialAlex KwokNo ratings yet
- Understanding Masticatory Function in Unilateral CrossbitesFrom EverandUnderstanding Masticatory Function in Unilateral CrossbitesNo ratings yet
- Cephalometric RadiographyDocument8 pagesCephalometric Radiographymkhaddas100% (3)
- Critical Review of Cephalometric RadiographyDocument26 pagesCritical Review of Cephalometric RadiographyEki Ryan SetiowatiNo ratings yet
- Functional OcclusionDocument8 pagesFunctional OcclusionNoor SolikhahNo ratings yet
- Treatment PlanningDocument28 pagesTreatment PlanningBimalKrishnaNo ratings yet
- Manual of Dental Practice 2014 Estonia: Council of European DentistsDocument10 pagesManual of Dental Practice 2014 Estonia: Council of European DentistsMohd GhausNo ratings yet
- Excellence in OrthodonticsDocument22 pagesExcellence in OrthodonticsAkram AlsharaeeNo ratings yet
- Abo GradingDocument11 pagesAbo GradingSonu RajuNo ratings yet
- Interceptive Orthodontics 1 / Orthodontic Courses by Indian Dental AcademyDocument44 pagesInterceptive Orthodontics 1 / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Comparison Between Surgically-Assisted Rapid Palatal Expansion (Sarpe) and Miniscrew-Assisted Rapid Palatal Expansion (Marpe) A Systematic ReviewDocument28 pagesComparison Between Surgically-Assisted Rapid Palatal Expansion (Sarpe) and Miniscrew-Assisted Rapid Palatal Expansion (Marpe) A Systematic Reviewaa bbNo ratings yet
- Hobo Technique PDFDocument8 pagesHobo Technique PDFAmar BimavarapuNo ratings yet
- Royal London Space AnalysisDocument47 pagesRoyal London Space AnalysisYusra ShaukatNo ratings yet
- Management of Class II Div IDocument13 pagesManagement of Class II Div Iapi-19840404No ratings yet
- Mandibular Incisor Extraction TherapyDocument10 pagesMandibular Incisor Extraction TherapyLeonardo LamimNo ratings yet
- Prostho Lec - OverdenturesDocument14 pagesProstho Lec - Overdenturesdrgayen6042No ratings yet
- Retention and RelapseDocument59 pagesRetention and RelapseAshwin ThejaswiNo ratings yet
- Myofunctional AppliancesDocument179 pagesMyofunctional AppliancesSwati PawarNo ratings yet
- 9 Cephalometric Analysis 2Document96 pages9 Cephalometric Analysis 2Mei Xiao100% (1)
- Soft Tissue Analysis: Dr. Ayushi Toley PG Ist YearDocument70 pagesSoft Tissue Analysis: Dr. Ayushi Toley PG Ist YearAyushi ToleyNo ratings yet
- DriftodonticsDocument2 pagesDriftodonticssweetieNo ratings yet
- Crossbite PosteriorDocument11 pagesCrossbite PosteriorrohmatuwidyaNo ratings yet
- Stem Cells in OrthodonticsDocument4 pagesStem Cells in OrthodonticsInternational Journal of Innovative Science and Research Technology100% (1)
- Etiology of Malocclusion & Habits: Dr. Biswaroop MohantyDocument74 pagesEtiology of Malocclusion & Habits: Dr. Biswaroop MohantynehanoopurNo ratings yet
- Centric Relation PDFDocument3 pagesCentric Relation PDFrekabiNo ratings yet
- Principles of Removable Partial Denture DesignDocument7 pagesPrinciples of Removable Partial Denture DesignAls EchanoNo ratings yet
- Cast AnalysisDocument9 pagesCast AnalysisAhmed SharabyNo ratings yet
- Bds Tutorial Overdentures 1Document7 pagesBds Tutorial Overdentures 1ikeuchi_ogawaNo ratings yet
- Diagnostic Limitations of Cephalometrics in OrthodonticsDocument6 pagesDiagnostic Limitations of Cephalometrics in OrthodonticsDevata RaviNo ratings yet
- A Beginners Guide To Lateral Cephalometric RadiographsDocument4 pagesA Beginners Guide To Lateral Cephalometric RadiographsClaudiaNo ratings yet
- 1 Objectives and Classification PD FayadDocument25 pages1 Objectives and Classification PD FayadMostafa FayadNo ratings yet
- Molar Distalization / Orthodontic Courses by Indian Dental AcademyDocument75 pagesMolar Distalization / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Dental Articulator & Face-Bow: ProsthodonticsDocument12 pagesDental Articulator & Face-Bow: ProsthodonticsPriyanka GandhiNo ratings yet
- 14 TMD Lecture - Tablet ViewDocument65 pages14 TMD Lecture - Tablet Viewdr666No ratings yet
- Mixed DentitionDocument49 pagesMixed Dentitiongnna norNo ratings yet
- Ret and RelapseDocument78 pagesRet and RelapseDeepshikha MandalNo ratings yet
- MARPE AbdAllah Bahaaa Ref NewDocument23 pagesMARPE AbdAllah Bahaaa Ref NewAya ElsayedNo ratings yet
- Cleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishraDocument9 pagesCleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishranomanNo ratings yet
- Andrews Keys of OcclusionDocument21 pagesAndrews Keys of OcclusionbhargaviNo ratings yet
- Aesthetics in Complete Denture - A REVIEWDocument2 pagesAesthetics in Complete Denture - A REVIEWInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Orthodontics 2 Lec M1 M2Document18 pagesOrthodontics 2 Lec M1 M2bambam1aNo ratings yet
- Class 3 Preadolecent Management by GowthamDocument53 pagesClass 3 Preadolecent Management by GowthamAbirami scientistNo ratings yet
- Lecture (17) Orthodontic Dentistry .: ساملا نانج د Orthopaedic Appliance in OrthodonticDocument3 pagesLecture (17) Orthodontic Dentistry .: ساملا نانج د Orthopaedic Appliance in Orthodonticاسراء فاضل مصطفى100% (1)
- 21 Biomechanics of Maxillary Expansion and Protraction in Class III Patients Copia 2Document2 pages21 Biomechanics of Maxillary Expansion and Protraction in Class III Patients Copia 2Vicente ContrerasNo ratings yet
- Space LossDocument5 pagesSpace LossAsma NawazNo ratings yet
- ImpressionDocument7 pagesImpressionAnnisa Nur AmalaNo ratings yet
- Smile Analysis: A Review Part IIDocument4 pagesSmile Analysis: A Review Part IIGustavoAndresGarciaNo ratings yet
- Evaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDocument6 pagesEvaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDiana Paola FontechaNo ratings yet
- Tweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisDocument56 pagesTweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisAnonymous 1uVifBp6100% (1)
- Goals of Orthodontic TreatmentDocument14 pagesGoals of Orthodontic TreatmentemanNo ratings yet
- Methods of Gaining Space 1. / Orthodontic Courses by Indian Dental AcademyDocument64 pagesMethods of Gaining Space 1. / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Growth QuesDocument8 pagesGrowth QuesShameer SFsNo ratings yet
- A Comparison Between Friction and FrictionlessDocument8 pagesA Comparison Between Friction and FrictionlessLiliana Aguilar Villarreal100% (1)
- SCOPE of DENTAL SUBJECTS and INTRODUCTION To ORAL ANATOMYDocument5 pagesSCOPE of DENTAL SUBJECTS and INTRODUCTION To ORAL ANATOMYLoreenNo ratings yet
- Comparative Study of Occlusal Contact Marking Indicators: Tanya P. BozhkovaDocument5 pagesComparative Study of Occlusal Contact Marking Indicators: Tanya P. BozhkovaMrinmayee ThakurNo ratings yet
- Aging White-Tailed Deer: Tooth & Jaw AnatomyDocument2 pagesAging White-Tailed Deer: Tooth & Jaw AnatomyDan ShepardNo ratings yet
- Kirschen2000 - The Royal London Space Planning - Part 1Document8 pagesKirschen2000 - The Royal London Space Planning - Part 1drgeorgejose7818100% (2)
- Cs LobodontiaDocument3 pagesCs LobodontiaInas ManurungNo ratings yet
- Complete Dentures: Arthur RussellDocument11 pagesComplete Dentures: Arthur RussellGermán PuigNo ratings yet
- Grade 4 - Ln.12 - Tongue and TeethDocument9 pagesGrade 4 - Ln.12 - Tongue and Teethpoornimaprabha90No ratings yet
- Oral Anatomy ReviewDocument10 pagesOral Anatomy ReviewYossy TjahyonoNo ratings yet
- Twin BlockDocument83 pagesTwin BlockBimalKrishnaNo ratings yet
- Amalgam Cavity Preparation Class 1Document51 pagesAmalgam Cavity Preparation Class 1Sourav GhoshNo ratings yet
- Bonding Brackets PDFDocument40 pagesBonding Brackets PDFMaria Yael75% (4)
- Role of Oral Musculature in Development of OcclusionDocument61 pagesRole of Oral Musculature in Development of OcclusionLakshmi Vamadevan0% (1)
- Evolution of Mammalian Molar Te - Osborn, Henry Fairfield, 1857-1Document272 pagesEvolution of Mammalian Molar Te - Osborn, Henry Fairfield, 1857-1AdrinianNo ratings yet
- Contacts and ContoursDocument99 pagesContacts and ContoursPooja Chaturvedi100% (4)
- Dental Vto MBTDocument10 pagesDental Vto MBTGabriela Castillo83% (6)
- The Andrews StrAight Wire Appliance PDFDocument198 pagesThe Andrews StrAight Wire Appliance PDFTati100% (1)
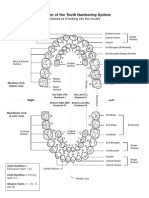
- Diagram of The Tooth Numbering SystemDocument1 pageDiagram of The Tooth Numbering Systemsaleh900No ratings yet
- Jones&Sadler 2012Document18 pagesJones&Sadler 2012Sidra ZahoorNo ratings yet
- Bucolingual Dimension of TeethDocument4 pagesBucolingual Dimension of TeethVicky Rahmaniah SyamsuryaNo ratings yet
- Etopic Eurption of The Firs Permanent MolarsDocument8 pagesEtopic Eurption of The Firs Permanent MolarsMartha Lia Castaño EcheverryNo ratings yet
- Plaque IndexDocument3 pagesPlaque Indexnuniatmanda100% (1)
- Occlusion 7Document10 pagesOcclusion 7krondanNo ratings yet
- Balanced Occlusion CD 2Document36 pagesBalanced Occlusion CD 2YJ Park100% (1)
- Question Bank Digestive SystemDocument9 pagesQuestion Bank Digestive SystemRonnith NandyNo ratings yet
- 1st BDS Oral Histology and Dental AnotomyDocument11 pages1st BDS Oral Histology and Dental AnotomyAmrutha Dasari100% (1)
- PREPROSTHODONTIC MOLAR INTRUSION BY MINI-IMPLANTS IN ADULT PATIENT-case ReportDocument1 pagePREPROSTHODONTIC MOLAR INTRUSION BY MINI-IMPLANTS IN ADULT PATIENT-case ReportVesna AndreevskaNo ratings yet
- Mammals Charcteristics Bio 117Document77 pagesMammals Charcteristics Bio 117MilitaryShellfishEyeNo ratings yet
- Concept of Normal OcclusionDocument39 pagesConcept of Normal OcclusionAlok Avinash100% (1)
- A Study of Root Canal Morphology of Human Primary Molars Using Computerised Tomography - An in Vitro Study Zoremchhingi, Joseph T, Varma B, Mungara J - J Indian Soc Pedod Prev DentDocument8 pagesA Study of Root Canal Morphology of Human Primary Molars Using Computerised Tomography - An in Vitro Study Zoremchhingi, Joseph T, Varma B, Mungara J - J Indian Soc Pedod Prev DentyeeruiNo ratings yet
- Anchorage: N.Mothi Krishna Ii Mds Department of OrthodonticsDocument83 pagesAnchorage: N.Mothi Krishna Ii Mds Department of OrthodonticsMothi KrishnaNo ratings yet