You might also like
- Acute Coronary Syndromes - HandoutDocument4 pagesAcute Coronary Syndromes - Handoutapi-641524095No ratings yet
- M10 Standards MVD Management DR C AtkinsDocument26 pagesM10 Standards MVD Management DR C Atkinsveterinaria87No ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction Algorithmjitendra magarNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- StrokeTIA Clinic Crozer 2022Document1 pageStrokeTIA Clinic Crozer 2022Franky QNo ratings yet
- Cardiology BookletDocument30 pagesCardiology Bookletali.khanfariplsNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction AlgorithmHan OWNo ratings yet
- Chest Pain Investigations and ManagementDocument4 pagesChest Pain Investigations and ManagementYY_1992No ratings yet
- ACLS Simulation ScenariosDocument14 pagesACLS Simulation ScenariosVanessa HermioneNo ratings yet
- Kegawatan Jantung - MeDocument41 pagesKegawatan Jantung - MeNam Min BinNo ratings yet
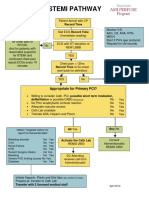
- STEMI Pathway FlowchartDocument2 pagesSTEMI Pathway FlowchartOlga Jadha CasmiraNo ratings yet
- Anti Coagulation For Surgery GuidelineDocument3 pagesAnti Coagulation For Surgery GuidelineNur SusiawantyNo ratings yet
- EMS Chest Pain ACS GuidelinesDocument1 pageEMS Chest Pain ACS GuidelinesJuanaly BadiolaNo ratings yet
- Acute Coronary Syndrome - YMDocument64 pagesAcute Coronary Syndrome - YMNirwanaNo ratings yet
- Shelf IM Video SlidesDocument69 pagesShelf IM Video SlidesRuth SanmooganNo ratings yet
- Acs Review - Student VersionDocument3 pagesAcs Review - Student Versionapi-549451092No ratings yet
- CCU HandoverDocument9 pagesCCU Handoverapi-192342497No ratings yet
- Chest Pain Cardiac Pre-Hospital ProtocolDocument1 pageChest Pain Cardiac Pre-Hospital Protocoleca nivlaNo ratings yet
- The PatientDocument9 pagesThe PatientJan Crizza Dale R. FrancoNo ratings yet
- QTC Flow Diagram With Medications Final Dec 17 A3 With LogosDocument1 pageQTC Flow Diagram With Medications Final Dec 17 A3 With LogosMelissa MurilloNo ratings yet
- Management of PatientsDocument19 pagesManagement of PatientsAmin MasromNo ratings yet
- Drug Induced Kel 5Document32 pagesDrug Induced Kel 5Nusaibah RomadhoniNo ratings yet
- ACS Management in Pandemic EraDocument56 pagesACS Management in Pandemic EraFatmawati nersNo ratings yet
- Chest Pain System - DisorderDocument1 pageChest Pain System - DisorderAA DDNo ratings yet
- Algorithm-ACLS ACS 200806 1Document1 pageAlgorithm-ACLS ACS 200806 1Kavya Shree100% (1)
- Clinical management of Covid19 updateDocument57 pagesClinical management of Covid19 updateJashveerBediNo ratings yet
- Section 2artfibDocument2 pagesSection 2artfibIain Tarrant-MurphyNo ratings yet
- ICU One Pager - Pulmonary Embolism RX PDFDocument1 pageICU One Pager - Pulmonary Embolism RX PDFAbdul RaufNo ratings yet
- Troponin PathwayDocument1 pageTroponin PathwayAllana AngelesNo ratings yet
- PASSMED MRCP MCQs-CARDIOLOGY & - 40 15& - 41 PDFDocument128 pagesPASSMED MRCP MCQs-CARDIOLOGY & - 40 15& - 41 PDFzeeshan ali100% (1)
- The Intern Pocket Card Surviving GraysDocument2 pagesThe Intern Pocket Card Surviving GraysKathleen Grace ManiagoNo ratings yet
- Clin Management Atrial Fibrillation Web AlgorithmDocument17 pagesClin Management Atrial Fibrillation Web AlgorithmArman PratomoNo ratings yet
- Management of Common Cases in Emergency MedicineDocument55 pagesManagement of Common Cases in Emergency MedicinemonpyitharNo ratings yet
- Medical Scenario 1Document42 pagesMedical Scenario 1murphy 1087No ratings yet
- Deep Vein ThrombosisDocument5 pagesDeep Vein Thrombosisampogison08No ratings yet
- Post PCI Care When To ReferDocument25 pagesPost PCI Care When To ReferRahmat HidayatullahNo ratings yet
- Periarestne AritmijeDocument10 pagesPeriarestne AritmijeMustafa ŠabićNo ratings yet
- Myocardial Infarction Concept MapDocument7 pagesMyocardial Infarction Concept Mapkarelclarke629280% (5)
- Dr. Rony M Santoso - ACS From Diagnosis To Long Term Treatment - Focus On Oral AntiplateletDocument25 pagesDr. Rony M Santoso - ACS From Diagnosis To Long Term Treatment - Focus On Oral AntiplateletluckyariadneeNo ratings yet
- COVID 19 Anticoagulation Algorithm Version Final 1.1Document2 pagesCOVID 19 Anticoagulation Algorithm Version Final 1.1Emi PuspitasariNo ratings yet
- Anti CoagulationDocument2 pagesAnti Coagulationsundance127No ratings yet
- Myocardial Infarction Management EDDocument1 pageMyocardial Infarction Management EDjljoioiuNo ratings yet
- CCU 2017 AntiplateletDocument22 pagesCCU 2017 AntiplateletDhinie NovianiNo ratings yet
- IMEDICS AKT Errors FINALDocument24 pagesIMEDICS AKT Errors FINALUmer AnwarNo ratings yet
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocument6 pagesAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNo ratings yet
- Pediatric Guidelines for MIS-CDocument8 pagesPediatric Guidelines for MIS-CSaima UmairNo ratings yet
- KawasakiDocument2 pagesKawasakiIvan WangNo ratings yet
- Acute Coronary SyndromeDocument5 pagesAcute Coronary Syndromecotten joeNo ratings yet
- Covid Flow ChartDocument1 pageCovid Flow ChartPeeaar Green Energy SolutionsNo ratings yet
- Cardiology I WorkbookDocument68 pagesCardiology I WorkbookPharmacist DinaNo ratings yet
- Cardio BBDocument73 pagesCardio BBايات عبدالرحمنNo ratings yet
- 2017 AHA Hypertension Guideline SummaryDocument16 pages2017 AHA Hypertension Guideline Summaryyassin mostafaNo ratings yet
- Esc Acs GuidelinesDocument62 pagesEsc Acs GuidelineszakiyaNo ratings yet
- SCE Practicaldiabetes - ElzohryDocument251 pagesSCE Practicaldiabetes - ElzohryAE100% (1)
- Update in Stroke ManagementDocument43 pagesUpdate in Stroke ManagementMuhidin AeNo ratings yet
- Acs 02152022 CjangDocument2 pagesAcs 02152022 Cjangapi-611971572No ratings yet
- Cardiac Emergency AMI GuideDocument34 pagesCardiac Emergency AMI GuideAdmin neuro-usu.idNo ratings yet
- MBTroponinGuidelin PDFDocument14 pagesMBTroponinGuidelin PDFBernadetta ViaNo ratings yet
- Algorithm For Perioperative Management of Anticoagulation1Document8 pagesAlgorithm For Perioperative Management of Anticoagulation1andi namirah100% (1)
- 32.3 Cough and Cold Medications in Pregnancy and LactationDocument8 pages32.3 Cough and Cold Medications in Pregnancy and LactationSahera Nurhidayah NasutionNo ratings yet
- 32.3 Cough and Cold Medications in Pregnancy and LactationDocument8 pages32.3 Cough and Cold Medications in Pregnancy and LactationSahera Nurhidayah NasutionNo ratings yet
- S JurnalDocument6 pagesS JurnalSahera Nurhidayah NasutionNo ratings yet
- Daftar Pustaka Bab IVDocument2 pagesDaftar Pustaka Bab IVSahera Nurhidayah NasutionNo ratings yet
- Molecules 16 02726 v3 PDFDocument17 pagesMolecules 16 02726 v3 PDFSahera Nurhidayah NasutionNo ratings yet
- Antiacne Nano Partikel PDFDocument10 pagesAntiacne Nano Partikel PDFLaiLi ImnidaNo ratings yet
- Interactions Between Your Drug1Document12 pagesInteractions Between Your Drug1Sahera Nurhidayah NasutionNo ratings yet
- Using NSAIDs in ChildrenDocument6 pagesUsing NSAIDs in ChildrenakyafauzanNo ratings yet
- IJPR - Volume Volume 5 - Issue Number 2 - Pages 149-152Document4 pagesIJPR - Volume Volume 5 - Issue Number 2 - Pages 149-152Sahera Nurhidayah NasutionNo ratings yet
- Ijprbs 434Document14 pagesIjprbs 434Sahera Nurhidayah NasutionNo ratings yet
- Juwita Ratna Dewi, Teti Estiasih, Dan Erni Sofia Murtini: Teties@yahoo - Co.idDocument10 pagesJuwita Ratna Dewi, Teti Estiasih, Dan Erni Sofia Murtini: Teties@yahoo - Co.idSahera Nurhidayah NasutionNo ratings yet
- Raja Et Al 2013Document7 pagesRaja Et Al 2013Sahera Nurhidayah NasutionNo ratings yet
- FUROSEMIDE 40MG TAB, 20MG AMP, 4MG/ML SYRUPDocument2 pagesFUROSEMIDE 40MG TAB, 20MG AMP, 4MG/ML SYRUPSahera Nurhidayah NasutionNo ratings yet
- Research Article Thermal Stability and Decomposition Kinetic Studies of Acyclovir and Zidovudine Drug CompoundsDocument7 pagesResearch Article Thermal Stability and Decomposition Kinetic Studies of Acyclovir and Zidovudine Drug CompoundsSahera Nurhidayah NasutionNo ratings yet
- Ijprbs 434Document14 pagesIjprbs 434Sahera Nurhidayah NasutionNo ratings yet
- Faring LaringDocument3 pagesFaring LaringSahera Nurhidayah NasutionNo ratings yet
- Volatile Constituents From The Leaves of Young and Old: Ailanthus Altissima (Mill.) Swingle TreeDocument9 pagesVolatile Constituents From The Leaves of Young and Old: Ailanthus Altissima (Mill.) Swingle TreeSahera Nurhidayah NasutionNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaSahera Nurhidayah NasutionNo ratings yet
- TrakeaDocument8 pagesTrakeaSahera Nurhidayah NasutionNo ratings yet
- FUROSEMIDE 40MG TAB, 20MG AMP, 4MG/ML SYRUPDocument2 pagesFUROSEMIDE 40MG TAB, 20MG AMP, 4MG/ML SYRUPSahera Nurhidayah NasutionNo ratings yet
- The Use of Botanical Extracts As Topical Skin-Lightening Agents For The Improvement of Skin Pigmentation DisordersDocument5 pagesThe Use of Botanical Extracts As Topical Skin-Lightening Agents For The Improvement of Skin Pigmentation Disordershamann511No ratings yet
- Pengertian Ion Exchange ChromatographyDocument7 pagesPengertian Ion Exchange ChromatographySahera Nurhidayah NasutionNo ratings yet
- High-Performance Liquid Chromatographic Determination of Arbutin in Skin-Whitening Creams and Medicinal Plant ExtractsDocument10 pagesHigh-Performance Liquid Chromatographic Determination of Arbutin in Skin-Whitening Creams and Medicinal Plant ExtractsSahera Nurhidayah NasutionNo ratings yet
- Hati 3Document10 pagesHati 3Sahera Nurhidayah NasutionNo ratings yet
- 1 PBDocument7 pages1 PBSahera Nurhidayah NasutionNo ratings yet
- EsofagusDocument6 pagesEsofagusSahera Nurhidayah NasutionNo ratings yet
- CH 3 Concept of ViscosityDocument11 pagesCH 3 Concept of ViscosityJenny ChenNo ratings yet
- DiazoDocument8 pagesDiazoParth DesaiNo ratings yet
- Ankit MangalDocument7 pagesAnkit MangalSahera Nurhidayah NasutionNo ratings yet
- Guidelines HPNDocument46 pagesGuidelines HPNSherif AbobakrNo ratings yet
- What Is Human PapillomavirusDocument7 pagesWhat Is Human PapillomavirusFerinaTarizaIINo ratings yet
- Nursing Care Plan Infection Bartholins Duct CystDocument1 pageNursing Care Plan Infection Bartholins Duct Cystderic100% (5)
- Angina: Angina:chest Pain Caused by Reduced Blood Flow To The Heart MuscleDocument11 pagesAngina: Angina:chest Pain Caused by Reduced Blood Flow To The Heart MuscleMohammed Falih HassanNo ratings yet
- Apollo Hospitals - First-World Health Care at Emerging - Market PricesDocument3 pagesApollo Hospitals - First-World Health Care at Emerging - Market PricesNaveen Chander Dhar100% (1)
- MicroscopeDocument8 pagesMicroscopeapi-3769525100% (2)
- Eye Surgery in Hot Climates 02Document25 pagesEye Surgery in Hot Climates 02Aulia CandraNo ratings yet
- Atlantis RXDocument2 pagesAtlantis RXJoe BridgeNo ratings yet
- Asas Perancangan Rekabentuk Fasiliti Kesihatan (F)Document82 pagesAsas Perancangan Rekabentuk Fasiliti Kesihatan (F)farahazuraNo ratings yet
- Maternity Magazine 2012 - 2013 PDFDocument212 pagesMaternity Magazine 2012 - 2013 PDFMaria Carolina LowenNo ratings yet
- NP5Document19 pagesNP5Jhouleen Angelika TamNo ratings yet
- Assessing Radial PulseDocument4 pagesAssessing Radial PulseMatthew RyanNo ratings yet
- 03 The Role of "Smart" Infusion Pumps in Patient Safety PDFDocument11 pages03 The Role of "Smart" Infusion Pumps in Patient Safety PDFSaravanan NallasivanNo ratings yet
- Signatory Guide To CREST Completion 2024Document5 pagesSignatory Guide To CREST Completion 2024junior docNo ratings yet
- Thesis Recovery After Cataract Surgery: Susanna Porela-TiihonenDocument40 pagesThesis Recovery After Cataract Surgery: Susanna Porela-TiihonenSaskia MediawatiNo ratings yet
- Assignment 2 Richa MaamDocument3 pagesAssignment 2 Richa MaamBrandon WaikhomNo ratings yet
- Hot Topic - Fluid ResuscitationDocument1 pageHot Topic - Fluid ResuscitationAnonymous fg5XXFOSj4No ratings yet
- Gap Co2 Cocc 2018Document9 pagesGap Co2 Cocc 2018Cesar Rivas CamposNo ratings yet
- Uterine InversionDocument14 pagesUterine InversionheenamaharjanNo ratings yet
- Muscle of The SoulDocument3 pagesMuscle of The SoulIrmak AlevNo ratings yet
- Nursing Care Plan for Skin IntegrityDocument3 pagesNursing Care Plan for Skin IntegrityCrystal Joy Misa100% (1)
- Medicine TT - Yr5-Batch 7 Rot-1, Gp-1Document10 pagesMedicine TT - Yr5-Batch 7 Rot-1, Gp-1Priya GKNo ratings yet
- Ethics Committee Resignation Letter 20161018Document3 pagesEthics Committee Resignation Letter 20161018CVRecordNo ratings yet
- Retained Placenta ManagementDocument4 pagesRetained Placenta ManagementDevanty AnggrainiNo ratings yet
- PERFORMANCE EVALUATION CRITERIADocument4 pagesPERFORMANCE EVALUATION CRITERIAmaryNo ratings yet
- Traumatic Brain Injury: Rehabilitation: Description of The Evidence Collection MethodDocument8 pagesTraumatic Brain Injury: Rehabilitation: Description of The Evidence Collection MethodDawud MuhammadNo ratings yet
- Chapter 4 of 10 - Kelsey HillDocument3 pagesChapter 4 of 10 - Kelsey HillspiritualbeingNo ratings yet
- HeartBeat Magazine1 Oktober 2017 PDFDocument32 pagesHeartBeat Magazine1 Oktober 2017 PDFMr. KINGNo ratings yet
- Coronary Artery Disease Nursing PresentationDocument32 pagesCoronary Artery Disease Nursing PresentationtanishaNo ratings yet
- 110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFDocument11 pages110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFaziz0% (1)