You might also like
- ABC of Intensive CareDocument49 pagesABC of Intensive CareCurro MirallesNo ratings yet
- ILCOR Part9 StrokeDocument5 pagesILCOR Part9 Strokedanayanto sumbungNo ratings yet
- Bab 198 Penggunaan Anti KoagulanDocument4 pagesBab 198 Penggunaan Anti KoagulanRaja Alfian IrawanNo ratings yet
- WHO Complete Hiv Report2009Document150 pagesWHO Complete Hiv Report2009danayanto sumbungNo ratings yet
- Update On ART-2010Document30 pagesUpdate On ART-2010danayanto sumbungNo ratings yet
- Art 1Document11 pagesArt 1danayanto sumbungNo ratings yet
- NVP Toxicity in Pregnant WomenDocument5 pagesNVP Toxicity in Pregnant Womendanayanto sumbungNo ratings yet
- 4-Mycobacterium Infection and HIVDocument45 pages4-Mycobacterium Infection and HIVdanayanto sumbungNo ratings yet
- 07 Antiretroviral Drug InteractionsDocument14 pages07 Antiretroviral Drug Interactionsdanayanto sumbungNo ratings yet
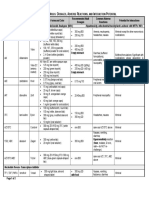
- Antiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction PotentialDocument2 pagesAntiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction Potentialdanayanto sumbungNo ratings yet
- 15 High Rate of Early Virological FailureDocument9 pages15 High Rate of Early Virological Failuredanayanto sumbungNo ratings yet
- AIDS Clinical CareDocument8 pagesAIDS Clinical Caredanayanto sumbungNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Infant and Young Child Feeding Guidelines: 2010Document10 pagesInfant and Young Child Feeding Guidelines: 2010Balaji_Rajaman_2280No ratings yet
- Httpslms - Naco.gov - Infrontendcontentnational Guidelines For PPTCT PDFDocument137 pagesHttpslms - Naco.gov - Infrontendcontentnational Guidelines For PPTCT PDFshlok jainNo ratings yet
- E-Poster PresentationDocument1 pageE-Poster PresentationOvamelia JulioNo ratings yet
- National Guidelines For PPTCT PDFDocument137 pagesNational Guidelines For PPTCT PDFJagannath Maale100% (1)
- Hiv/Aids: Prof. Dr. Ram Sharan Mehta Medical-Surgical Nursing DepartmentDocument196 pagesHiv/Aids: Prof. Dr. Ram Sharan Mehta Medical-Surgical Nursing DepartmentDavid Sergio Salas VargasNo ratings yet
- Drugs Acting On Immune SystemDocument6 pagesDrugs Acting On Immune SystemSORENI SORENINo ratings yet
- Neofax 2020 (430-791)Document362 pagesNeofax 2020 (430-791)Paola Yelitza Rodriguez TorreNo ratings yet
- Hyper CvadDocument5 pagesHyper CvadAmr MuhammedNo ratings yet
- ZIM ART Guidelines 2016 - Review FinalDocument136 pagesZIM ART Guidelines 2016 - Review FinalCollen LihakaNo ratings yet
- HIV Infectious DiseasesDocument50 pagesHIV Infectious Diseasesabdul qayyumNo ratings yet
- National AIDS Control Programme: Debajani NayakDocument66 pagesNational AIDS Control Programme: Debajani NayakGandimareiNo ratings yet
- CABULADocument26 pagesCABULAYassboy MsdNo ratings yet
- Nevirapine Drug .Document11 pagesNevirapine Drug .AminaNo ratings yet
- Manajemen Hiv.1Document92 pagesManajemen Hiv.1Ariestha Teza AdipratamaNo ratings yet
- Botswana National Hiv Aids Treatment GuidelinesDocument140 pagesBotswana National Hiv Aids Treatment GuidelinesMandisa Ndlovu TenegoNo ratings yet
- HIV/Infectious Diseases: Curtis L - Smith, Pharm. D., BCPSDocument42 pagesHIV/Infectious Diseases: Curtis L - Smith, Pharm. D., BCPSandirio7486No ratings yet
- Pharma FT T&DDocument5 pagesPharma FT T&DAastha JainNo ratings yet
- Management of Infants BornDocument6 pagesManagement of Infants BornDiana FlorezNo ratings yet
- PHCP FinalsDocument43 pagesPHCP FinalsEli ChuaNo ratings yet
- Cipla LTD Company ProfileDocument13 pagesCipla LTD Company ProfileAdnan Ejaz33% (3)
- Management of HIV in Pregnant WomenDocument53 pagesManagement of HIV in Pregnant Womenumiraihana1No ratings yet
- MTRH Medicine GuidelinesDocument42 pagesMTRH Medicine Guidelineskevincavin82No ratings yet
- Cipla Corporate Presentation PDFDocument30 pagesCipla Corporate Presentation PDFAbhay SrivastavaNo ratings yet
- Rwanda Medicaments EssentielsDocument85 pagesRwanda Medicaments EssentielsportosinNo ratings yet
- Presented By,: Aneeta Anna Abraham I Year M Pharm Pharmacy PracticeDocument31 pagesPresented By,: Aneeta Anna Abraham I Year M Pharm Pharmacy PracticeREETHUNo ratings yet
- Paediatric Dosage of Some Drugs-1Document45 pagesPaediatric Dosage of Some Drugs-1JaneNo ratings yet
- Antiretroviral DrugsDocument60 pagesAntiretroviral DrugsDeribe BekeleNo ratings yet
- Navirapine DrugDocument38 pagesNavirapine DrugAminaNo ratings yet
- Hiv in PregnancyDocument52 pagesHiv in PregnancyKirandeep ParmarNo ratings yet
- Cureus 0008 000000000515 PDFDocument12 pagesCureus 0008 000000000515 PDFDini WurnaningNo ratings yet