You might also like
- Systems AnalystDocument2 pagesSystems Analystsandeep_nagar29No ratings yet
- Sweet Success: Knowledge and Quick-Skills in Thirty MinutesFrom EverandSweet Success: Knowledge and Quick-Skills in Thirty MinutesNo ratings yet
- Teachers Application FormDocument6 pagesTeachers Application FormVivekananda Kendra Shiksha Prasar Vibhag100% (1)
- Application Forms and Guidelines For Applicants - VKSPV-Teachers' Interview - 2020-21Document6 pagesApplication Forms and Guidelines For Applicants - VKSPV-Teachers' Interview - 2020-21Vivekananda Kendra80% (5)
- Application Form For Post of Teacher Vkvapt PDFDocument3 pagesApplication Form For Post of Teacher Vkvapt PDFNeeldeep ChakrabortyNo ratings yet
- NsicDocument2 pagesNsicpravinNo ratings yet
- Preliminary Credit Facility Application Form - PostGSTDocument10 pagesPreliminary Credit Facility Application Form - PostGSThs404671No ratings yet
- Admission Application FormDocument2 pagesAdmission Application FormSatyajit DharNo ratings yet
- Admission Notification Mphil 2023-25-2-1Document1 pageAdmission Notification Mphil 2023-25-2-1DharikaNo ratings yet
- Ubth Application Form OriginalDocument3 pagesUbth Application Form OriginalTaiwo Chris Awoyemi100% (1)
- MedicalOfficerAdvertisementOfPanipat 15032024Document9 pagesMedicalOfficerAdvertisementOfPanipat 15032024keshavmittal7015No ratings yet
- STSANDSTLSADVERTISEMENTOfPanipat 1503024Document9 pagesSTSANDSTLSADVERTISEMENTOfPanipat 1503024keshavmittal7015No ratings yet
- DHFWS Panipat ANM Posts Notification and Application Form PDFDocument9 pagesDHFWS Panipat ANM Posts Notification and Application Form PDFchirag NarangNo ratings yet
- Position Applied For I. Personal Identity: Pas FotoDocument4 pagesPosition Applied For I. Personal Identity: Pas Fototri188No ratings yet
- Application Forms and Guidelines For Applicants For VKSPV Teachers Interview 2023-24Document6 pagesApplication Forms and Guidelines For Applicants For VKSPV Teachers Interview 2023-24Vivekananda KendraNo ratings yet
- Sector 30-C, Chandigarh: Csir-Central Scientific Instruments OrganisationDocument2 pagesSector 30-C, Chandigarh: Csir-Central Scientific Instruments OrganisationSudhanshu ShekharNo ratings yet
- ApplicationDocument2 pagesApplicationPreetam RajkeNo ratings yet
- Dr. Babasaheb Ambedkar Open University: Assistant Professor SanskritDocument5 pagesDr. Babasaheb Ambedkar Open University: Assistant Professor Sanskritprachi patelNo ratings yet
- RESIDENT NMC - Declaration - Form - Revised - 2020-2021Document6 pagesRESIDENT NMC - Declaration - Form - Revised - 2020-2021Riya TapadiaNo ratings yet
- Bachelor of Fine Arts (B.F.A.) 4 Years (8 Semesters) Girls) : (BoysDocument4 pagesBachelor of Fine Arts (B.F.A.) 4 Years (8 Semesters) Girls) : (BoysPrakashNo ratings yet
- FormDocument3 pagesFormpukhrajgehlotNo ratings yet
- Registration Form: Please Affix A Passport Size PhotoDocument2 pagesRegistration Form: Please Affix A Passport Size PhotoJayachandra Reddy AnnavaramNo ratings yet
- 3 Application Form NT 2019 PDFDocument10 pages3 Application Form NT 2019 PDFNallanki Raja KumarNo ratings yet
- Proposal For Membership of The Association: EmailDocument2 pagesProposal For Membership of The Association: EmailAnonymous mKIr49No ratings yet
- Education Division Bio-Data Form422176620191220Document3 pagesEducation Division Bio-Data Form422176620191220Nani VenkeyNo ratings yet
- SNM BGSScholarshipScheme2023 24form ANNEXURE IIDocument5 pagesSNM BGSScholarshipScheme2023 24form ANNEXURE IIHarshad NaleNo ratings yet
- JOB APPLICATION FORM For BS 1 To BS 16Document3 pagesJOB APPLICATION FORM For BS 1 To BS 16Momina SaadNo ratings yet
- App FormatDocument2 pagesApp FormatDarwin SteniNo ratings yet
- UG Admission Form 2010Document5 pagesUG Admission Form 2010Sevak AmitNo ratings yet
- Jobs App Form GeneralDocument1 pageJobs App Form GeneralEngr Shah JeeNo ratings yet
- Application Form For CandidateDocument7 pagesApplication Form For CandidateShanmuga KannanNo ratings yet
- Session: January, 2008: Dy. No. - DateDocument11 pagesSession: January, 2008: Dy. No. - Datemahesh100% (1)
- Application Form: To Admin Officer (Estt) P.O.Box No. 2241 Islamabad Post Applied ForDocument1 pageApplication Form: To Admin Officer (Estt) P.O.Box No. 2241 Islamabad Post Applied ForAbdul munirNo ratings yet
- Application Form For Engagement of Young Professionals (Yp) On Contract BasisDocument1 pageApplication Form For Engagement of Young Professionals (Yp) On Contract BasispujaadiNo ratings yet
- Comtax Ja PDF Form 19 Opt1 New 0 PDFDocument2 pagesComtax Ja PDF Form 19 Opt1 New 0 PDFKishore BarmanNo ratings yet
- 42bb5 c1f75 Application Form For Mos DoctorsDocument2 pages42bb5 c1f75 Application Form For Mos DoctorsDanish KhanNo ratings yet
- Notification CCRUM Various Vacancy PostsDocument5 pagesNotification CCRUM Various Vacancy PostsRajkumarNo ratings yet
- 574808059performa ContractualDocument2 pages574808059performa ContractualDev YadavNo ratings yet
- Application Form2 ILs Bhubaneswar RA SRF PostsDocument2 pagesApplication Form2 ILs Bhubaneswar RA SRF PostsjatinyadavblogNo ratings yet
- Wa0006 PDFDocument6 pagesWa0006 PDFsivaNo ratings yet
- Project AssistantDocument1 pageProject AssistantGarapati JayasriNo ratings yet
- Application Form1 Dec 2010Document3 pagesApplication Form1 Dec 2010Kiran RokadeNo ratings yet
- 2 Application Form Study in SathyabamaDocument2 pages2 Application Form Study in SathyabamaVENKATESH ALISHAMNo ratings yet
- 4 TPS Admin 104 Job Application Form Ministerial and Admin StaffDocument2 pages4 TPS Admin 104 Job Application Form Ministerial and Admin Staffaminaamin.aiou48No ratings yet
- Hidayatullah National Law University: Admission FormDocument3 pagesHidayatullah National Law University: Admission FormVishrut PNo ratings yet
- Proforma For Application: (I, II, III)Document4 pagesProforma For Application: (I, II, III)sunil_3679No ratings yet
- Fee Concession ProformaDocument1 pageFee Concession ProformaKashish MahajanNo ratings yet
- Tech 1Document4 pagesTech 1thkomal0914No ratings yet
- Shri Vishwakarma Skill University: Admission Form For Phd. Session: - 2020-21Document2 pagesShri Vishwakarma Skill University: Admission Form For Phd. Session: - 2020-21Ravish YadavNo ratings yet
- University of Mumbai: Admission FormDocument4 pagesUniversity of Mumbai: Admission FormMohaseen Khan S LNo ratings yet
- Undergraduate Application Form-23022022Document2 pagesUndergraduate Application Form-23022022bongisebodgeNo ratings yet
- Application Form For Commission in The RFDocument4 pagesApplication Form For Commission in The RFMary Ann Jennifer AfagaNo ratings yet
- Application Form: Designation From Date To Date Name of OrganizationDocument1 pageApplication Form: Designation From Date To Date Name of OrganizationYasir BalochNo ratings yet
- Arbiter Refresher Entry FormDocument1 pageArbiter Refresher Entry FormregistermailNo ratings yet
- Application Form For Enlistment Into Paf Reserve ForceDocument4 pagesApplication Form For Enlistment Into Paf Reserve ForceXadNo ratings yet
- Admission Form SNTCSSC Batch 2024Document3 pagesAdmission Form SNTCSSC Batch 2024Dhruba PatraNo ratings yet
- Compulsory Govt Service Notification 2022Document3 pagesCompulsory Govt Service Notification 2022Vikram ThakurNo ratings yet
- Hidayatullah National Law University: Admission FormDocument2 pagesHidayatullah National Law University: Admission Formvijaya choudharyNo ratings yet
- Obc 9050Document3 pagesObc 9050Ankit PalNo ratings yet
- Cover Letter Journal of Food Processing and PreservationDocument1 pageCover Letter Journal of Food Processing and PreservationStevenCarlNo ratings yet
- A Study of The Relationship Between Student Social Networks and Sense of CommunityDocument15 pagesA Study of The Relationship Between Student Social Networks and Sense of CommunityTaban KhalidNo ratings yet
- Formulation Optimization of A Palm-Based Nanoemulsion System Containing LevodopaDocument16 pagesFormulation Optimization of A Palm-Based Nanoemulsion System Containing LevodopaAnton MelcherNo ratings yet
- Apj Abdul KalamDocument16 pagesApj Abdul Kalamamanblr12100% (2)
- The Role of Organizational Citizenship Behavior OnDocument16 pagesThe Role of Organizational Citizenship Behavior OnMd Shawfiqul IslamNo ratings yet
- 6 Adult Learning Theories - Put Theory Into PracticeDocument15 pages6 Adult Learning Theories - Put Theory Into PracticeAmba Lrcfools InfosNo ratings yet
- A8 Maersk CaseDocument5 pagesA8 Maersk CaseSuduNo ratings yet
- Scope Insensitivity in Child's Health Risk Reduction: A Comparison of Damage Schedule and Choice Experiment MethodsDocument32 pagesScope Insensitivity in Child's Health Risk Reduction: A Comparison of Damage Schedule and Choice Experiment MethodsJose DGNo ratings yet
- KCL Mediating Construction CompleteDocument95 pagesKCL Mediating Construction CompleteStefania G. LaviniaNo ratings yet
- Educational Spaces QualityDocument7 pagesEducational Spaces QualityDanaNo ratings yet
- GOM Brochure Training enDocument28 pagesGOM Brochure Training enEmerson CruzNo ratings yet
- Research Group 10Document8 pagesResearch Group 10Louielyn MagalangNo ratings yet
- Curriculum Vitae: Full Name Date of Birth Sex Email AddressDocument2 pagesCurriculum Vitae: Full Name Date of Birth Sex Email AddressDiki WiganNo ratings yet
- T TESTDocument24 pagesT TESTanmolgarg129No ratings yet
- State Level Syllabus of Sociology For Undergraduate LevelDocument10 pagesState Level Syllabus of Sociology For Undergraduate LevelKrishna AhujaNo ratings yet
- Increasing Support For Evidence-Based Policing A Complexity TheoDocument153 pagesIncreasing Support For Evidence-Based Policing A Complexity TheomaolewiNo ratings yet
- Presentation and ScriptsDocument3 pagesPresentation and ScriptsJireh AlveyraNo ratings yet
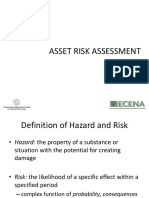
- Assesment RiskDocument69 pagesAssesment RiskAhmad MaulidiNo ratings yet
- Bird Strike - A ReviewDocument20 pagesBird Strike - A ReviewApolloNo ratings yet
- Why Appraisal Is Not Utterly' Useless and Why It's Not The Way To Go EitherDocument2 pagesWhy Appraisal Is Not Utterly' Useless and Why It's Not The Way To Go Eitherghoshtapan4321No ratings yet
- CH 18Document570 pagesCH 18mrlyNo ratings yet
- Coaching Your Employees Ed Batista HBR Webinar Summary PDFDocument7 pagesCoaching Your Employees Ed Batista HBR Webinar Summary PDFDam To Minh100% (1)
- Literature Review: Prof M. Sandada 0772363753 Msandada@uzbusinessschool - Uz.ac - ZW Uzbusiness School Office No. 7Document12 pagesLiterature Review: Prof M. Sandada 0772363753 Msandada@uzbusinessschool - Uz.ac - ZW Uzbusiness School Office No. 7Tinotenda FredNo ratings yet
- Use of PEARL in Assessing TRL AKB LDocument28 pagesUse of PEARL in Assessing TRL AKB LVikas Jawaria100% (1)
- Calibration ProcedureDocument2 pagesCalibration ProcedureSairam Edupuganti100% (1)
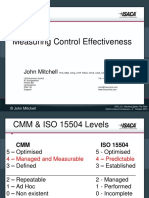
- Measuring Control Effectiveness - John MitchellDocument19 pagesMeasuring Control Effectiveness - John MitchellShah Maqsumul Masrur TanviNo ratings yet
- Analyzing The Effectiveness of Reward Management System On Employee Performance Through The Mediating Role of Employee MotivationDocument12 pagesAnalyzing The Effectiveness of Reward Management System On Employee Performance Through The Mediating Role of Employee MotivationRenz Dela Cruz ArellanoNo ratings yet
- Iep Scavenger HuntDocument2 pagesIep Scavenger Huntapi-31803486275% (4)
- Math T Coursework 2020 Sem 3Document14 pagesMath T Coursework 2020 Sem 3Melody OngNo ratings yet
- Simplified Guide To Fingerprint AnalysisDocument13 pagesSimplified Guide To Fingerprint AnalysisPRINCES ALLEN MATULACNo ratings yet
- Essential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsFrom EverandEssential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsRating: 3 out of 5 stars3/5 (2)
- Dictionary of Legal Terms: Definitions and Explanations for Non-LawyersFrom EverandDictionary of Legal Terms: Definitions and Explanations for Non-LawyersRating: 5 out of 5 stars5/5 (2)
- Nolo's Deposition Handbook: The Essential Guide for Anyone Facing or Conducting a DepositionFrom EverandNolo's Deposition Handbook: The Essential Guide for Anyone Facing or Conducting a DepositionRating: 5 out of 5 stars5/5 (1)
- Legal Writing in Plain English: A Text with ExercisesFrom EverandLegal Writing in Plain English: A Text with ExercisesRating: 3 out of 5 stars3/5 (2)
- The Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyFrom EverandThe Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyRating: 5 out of 5 stars5/5 (2)
- A Student's Guide to Law School: What Counts, What Helps, and What MattersFrom EverandA Student's Guide to Law School: What Counts, What Helps, and What MattersRating: 5 out of 5 stars5/5 (4)
- Torts: QuickStudy Laminated Reference GuideFrom EverandTorts: QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- So You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolFrom EverandSo You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolNo ratings yet
- Employment Law: a Quickstudy Digital Law ReferenceFrom EverandEmployment Law: a Quickstudy Digital Law ReferenceRating: 1 out of 5 stars1/5 (1)
- Nolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsFrom EverandNolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsRating: 4 out of 5 stars4/5 (18)
- Flora and Vegetation of Bali Indonesia: An Illustrated Field GuideFrom EverandFlora and Vegetation of Bali Indonesia: An Illustrated Field GuideRating: 5 out of 5 stars5/5 (2)
- Admissibility of Expert Witness TestimonyFrom EverandAdmissibility of Expert Witness TestimonyRating: 5 out of 5 stars5/5 (1)
- How to Make Patent Drawings: Save Thousands of Dollars and Do It With a Camera and Computer!From EverandHow to Make Patent Drawings: Save Thousands of Dollars and Do It With a Camera and Computer!Rating: 5 out of 5 stars5/5 (1)
- Legal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersFrom EverandLegal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersNo ratings yet
- Legal Writing in Plain English, Third Edition: A Text with ExercisesFrom EverandLegal Writing in Plain English, Third Edition: A Text with ExercisesNo ratings yet
- Busted!: Drug War Survival Skills and True Dope DFrom EverandBusted!: Drug War Survival Skills and True Dope DRating: 3.5 out of 5 stars3.5/5 (7)