You might also like
- Safety Data Sheet Rapid Fixer: According To Regulation (EC) No 1907/2006, Annex II, As AmendedDocument14 pagesSafety Data Sheet Rapid Fixer: According To Regulation (EC) No 1907/2006, Annex II, As AmendedabrianNo ratings yet
- Unclos TerjemahanDocument172 pagesUnclos TerjemahanHartotok VipnetNo ratings yet
- Riviwanto 2019 IOP Conf. Ser. Earth Environ. Sci. 314 012086Document11 pagesRiviwanto 2019 IOP Conf. Ser. Earth Environ. Sci. 314 012086abrianNo ratings yet
- Template Contoh HSE PlanDocument31 pagesTemplate Contoh HSE PlanAndi MuliadiNo ratings yet
- Safety Data Sheet Rapid Fixer: According To Regulation (EC) No 1907/2006, Annex II, As AmendedDocument14 pagesSafety Data Sheet Rapid Fixer: According To Regulation (EC) No 1907/2006, Annex II, As AmendedabrianNo ratings yet
- Towards A Science of Rabies Elimination: Commentary Open AccessDocument3 pagesTowards A Science of Rabies Elimination: Commentary Open AccessabrianNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 10 PulmunologyDocument111 pages10 PulmunologyJeet JainNo ratings yet
- QR Management of Neonatal Jaundice (Second Edition) PDFDocument8 pagesQR Management of Neonatal Jaundice (Second Edition) PDFOlayinka AwofoduNo ratings yet
- Mental Health AwarenessDocument13 pagesMental Health AwarenessMaxine AguilarNo ratings yet
- A-Plus Early Criticalcare Brochure Full 20130529 FinalDocument18 pagesA-Plus Early Criticalcare Brochure Full 20130529 Finalnusthe2745No ratings yet
- Osteomyelitis: ClassificationDocument5 pagesOsteomyelitis: Classificationthanuja mathewNo ratings yet
- EBM Case Write Up - To Rule Out MERS COVDocument5 pagesEBM Case Write Up - To Rule Out MERS COVFaiz TaqiuNo ratings yet
- Reasons Why You Should Get The COVID 19 VaccineDocument4 pagesReasons Why You Should Get The COVID 19 VaccineShane Patrick PanilagNo ratings yet
- Coding KKPMT CardioDocument6 pagesCoding KKPMT CardioNadlifahHidayatiNo ratings yet
- Department of Education Division of Lanao Del Norte Felisa Villoria Bond Elementary SchoolDocument11 pagesDepartment of Education Division of Lanao Del Norte Felisa Villoria Bond Elementary SchoolSARAH JEAN CABUGNASONNo ratings yet
- Bulimia NervosaDocument19 pagesBulimia NervosaAmoroso, Marian Corneth D.No ratings yet
- Phenylketonur IA: Done byDocument27 pagesPhenylketonur IA: Done byAsfoor gake1100% (1)
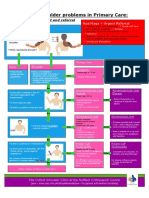
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertNo ratings yet
- Mkpdp1035 : Name Lab No. Refby: Gender: Report Status Collected Mkpdp1035 Male DR - Veena BoraDocument2 pagesMkpdp1035 : Name Lab No. Refby: Gender: Report Status Collected Mkpdp1035 Male DR - Veena Borachetan bhagatNo ratings yet
- Jan Marc S. Karganilla 10-Newton: Parkinson's Disease Cerebral Palsy AtaxiaDocument2 pagesJan Marc S. Karganilla 10-Newton: Parkinson's Disease Cerebral Palsy Ataxia박우진No ratings yet
- Wadh0022 Assignment 4 With FeedbackDocument39 pagesWadh0022 Assignment 4 With FeedbackViswaVittal's TheHiddenWorldNo ratings yet
- The Gram - Negative Bacilli of Medical ImportantDocument22 pagesThe Gram - Negative Bacilli of Medical ImportantVatha NaNo ratings yet
- Chapter 18 - Liver and Biliary TractDocument18 pagesChapter 18 - Liver and Biliary TractAgnieszka WisniewskaNo ratings yet
- Why Even Fully Vaccinated Older People Are at High Risk For Severe COVID-19Document3 pagesWhy Even Fully Vaccinated Older People Are at High Risk For Severe COVID-19Jorge Vivas SantistebanNo ratings yet
- Absence of Responsible Member and Financial ConstraintsDocument2 pagesAbsence of Responsible Member and Financial ConstraintsFavor ColaNo ratings yet
- TOEIC - Intermediate Anatomy, Health, and Beauty Vocabulary Set 2 PDFDocument6 pagesTOEIC - Intermediate Anatomy, Health, and Beauty Vocabulary Set 2 PDFNguraIrunguNo ratings yet
- PTS Ganjil Kelas 10 LMDocument7 pagesPTS Ganjil Kelas 10 LMAulia FatihaNo ratings yet
- NCP - Risk For InfectionDocument3 pagesNCP - Risk For InfectionSiergs Smith Gervacio100% (3)
- Nclex Questions Chap 23 38Document162 pagesNclex Questions Chap 23 38Sophia Rose Delos Santos100% (2)
- Chest Pain CasesDocument74 pagesChest Pain Casesmedpedshospitalist100% (2)
- Sexually Transmitted Diseases (STDS) Tahir Kundki 6Document22 pagesSexually Transmitted Diseases (STDS) Tahir Kundki 6shahrukhziaNo ratings yet
- Knowledge Attitudes and Testing Preferences For Herpes Simplex Virus Infections Among Undergraduate Students at A Large University in Los AngelesDocument7 pagesKnowledge Attitudes and Testing Preferences For Herpes Simplex Virus Infections Among Undergraduate Students at A Large University in Los AngelessesiaNo ratings yet
- Askep IsosDocument3 pagesAskep IsosWayan SugitaNo ratings yet
- Statistical Analysis and Data Visualization of Indonesia and Malaysia Sars Cov-2 MetadataDocument10 pagesStatistical Analysis and Data Visualization of Indonesia and Malaysia Sars Cov-2 MetadataSahalS MNo ratings yet
- APBCS APBECS FAQ v3 CleanDocument14 pagesAPBCS APBECS FAQ v3 CleanLee MingNo ratings yet
- Secondary Data Analysis of ThiruvallurDocument10 pagesSecondary Data Analysis of ThiruvallurSimbakutty VenkataramananNo ratings yet