You might also like
- Table Final Website IHU 09 04 2020 PDFDocument1 pageTable Final Website IHU 09 04 2020 PDFArthur HenriqueNo ratings yet
- Covid-19 Death Analysis Among Vaccinated 1Document3 pagesCovid-19 Death Analysis Among Vaccinated 1බූ බූNo ratings yet
- COVID-19 Weekly Report: Figure 1. Reported Signs and Symptoms For All Confirmed COVID 19 Cases (N 1099)Document3 pagesCOVID-19 Weekly Report: Figure 1. Reported Signs and Symptoms For All Confirmed COVID 19 Cases (N 1099)mscribariaNo ratings yet
- COVID-19 Mass Vaccination Analysis 3-22-2021-UPDATEDocument11 pagesCOVID-19 Mass Vaccination Analysis 3-22-2021-UPDATEDavid IbanezNo ratings yet
- Dampak Ekonomi Akibat TB (The Economic Impacts of Tuberculosis)Document23 pagesDampak Ekonomi Akibat TB (The Economic Impacts of Tuberculosis)indosquad피곤한No ratings yet
- 2009 Ctuw Research Final EmbargoedDocument14 pages2009 Ctuw Research Final EmbargoedMarco RamirezNo ratings yet
- SLS TrendsDocument29 pagesSLS TrendsSohaib Mohammad KhanNo ratings yet
- ProtecciónDocument10 pagesProtecciónTatiana Castro HernándezNo ratings yet
- Population, Hiv/ Aids, Human Right: Group Member 1. Mishul 2. Diksha 3. NitinDocument13 pagesPopulation, Hiv/ Aids, Human Right: Group Member 1. Mishul 2. Diksha 3. NitinMishul GuptaNo ratings yet
- Letters: Pneumonia in Children Presenting To The Emergency Department With An Asthma ExacerbationDocument3 pagesLetters: Pneumonia in Children Presenting To The Emergency Department With An Asthma ExacerbationRhahima SyafrilNo ratings yet
- Need Assessment 2008Document3 pagesNeed Assessment 2008Peer Coach Academy Colorado100% (2)
- Characteristics of Sars-Cov-2 Patients Dying in Italy Report Based On Available Data On May 7, 2020Document6 pagesCharacteristics of Sars-Cov-2 Patients Dying in Italy Report Based On Available Data On May 7, 2020RafiamNo ratings yet
- Pengendalian PTM Terpadu (Deteksi Dini, Pemantauan Faktor Risiko Melalui Konseling PTM)Document2 pagesPengendalian PTM Terpadu (Deteksi Dini, Pemantauan Faktor Risiko Melalui Konseling PTM)Amelia AmelNo ratings yet
- 1998 Methodology Report - Standard Error Tables (Lifetime Substance Use - Secondary Grades)Document4 pages1998 Methodology Report - Standard Error Tables (Lifetime Substance Use - Secondary Grades)Texas School Survey of Drug and Alcohol UseNo ratings yet
- KY COVID-19 Daily SummaryDocument6 pagesKY COVID-19 Daily SummaryThiago PresaNo ratings yet
- The Specialty Food Buyer ProfileDocument2 pagesThe Specialty Food Buyer ProfileJohn Henry WellsNo ratings yet
- Statistical POwerDocument35 pagesStatistical POwerWawex DavisNo ratings yet
- EPI BangladeshDocument4 pagesEPI BangladeshToufiq Rahman100% (1)
- Demographic data frequenciesDocument4 pagesDemographic data frequenciesGenesa Buen A. PolintanNo ratings yet
- SoCal's UW Step 2 CK EOs (UTD 10 Nov)Document292 pagesSoCal's UW Step 2 CK EOs (UTD 10 Nov)JJ0% (1)
- Health Research Agenda Setting in Region 1Document14 pagesHealth Research Agenda Setting in Region 1Maureen Joy Cascayan EspirituNo ratings yet
- Daily Summary: 18 Duplicates and Records Not Meeting Case Criteria Removed Since Last ReportDocument6 pagesDaily Summary: 18 Duplicates and Records Not Meeting Case Criteria Removed Since Last ReportJm2345234029No ratings yet
- 1 The High Risk MotherDocument161 pages1 The High Risk MotherRaquel M. MendozaNo ratings yet
- AguilarDocument5 pagesAguilarEmmánNo ratings yet
- BolinaoDocument8 pagesBolinaoEmmánNo ratings yet
- Final Article Rcog 31 Mei Jam 4 PagiDocument11 pagesFinal Article Rcog 31 Mei Jam 4 Pagikusumavk semarangNo ratings yet
- 1 s2.0 S0300289621001745 mmc2Document2 pages1 s2.0 S0300289621001745 mmc2aris dwiprasetyaNo ratings yet
- MMC 1Document5 pagesMMC 1Oki OzoraNo ratings yet
- Contribution of EclampsiaDocument25 pagesContribution of EclampsiaUsha AnengaNo ratings yet
- COMMODITY PRICE DASHBOARD - MAY 2019Document9 pagesCOMMODITY PRICE DASHBOARD - MAY 2019mihaiNo ratings yet
- Children Entering Foster Care in North Carolina - SFY 2013-2017Document2 pagesChildren Entering Foster Care in North Carolina - SFY 2013-2017SarahNo ratings yet
- Results Group 1-2Document7 pagesResults Group 1-2Areenub ArshadNo ratings yet
- Price Dashboard: No 116 - January 2022 EditionDocument9 pagesPrice Dashboard: No 116 - January 2022 EditionNebojsa RadulovicNo ratings yet
- OMS Head Circumference Percentiles Calculator for Infant AgeDocument1 pageOMS Head Circumference Percentiles Calculator for Infant AgeSolhana MendietaNo ratings yet
- CINA Deluxe DQP SSFs For Prostate Cancer 2011 2015Document6 pagesCINA Deluxe DQP SSFs For Prostate Cancer 2011 2015MayNo ratings yet
- Exercise 7Document4 pagesExercise 7Humpy DumpyNo ratings yet
- Orange County DemographicsDocument2 pagesOrange County DemographicsionspinNo ratings yet
- Eu 021 PDFDocument9 pagesEu 021 PDFempower93 empower93No ratings yet
- Apendix B Age Bracket in The Population of Santa RosaDocument2 pagesApendix B Age Bracket in The Population of Santa RosaLaarni S. TalusanNo ratings yet
- Anemia en RNDocument21 pagesAnemia en RNDaniel Martinez DiazNo ratings yet
- Priority Disease ReportDocument24 pagesPriority Disease ReportalirrehmanNo ratings yet
- BarangayDocument2 pagesBarangayDan Bryan AndalanNo ratings yet
- Supplementary data and analyses for "Cardiovascular disease, drug therapy, and mortality in Covid-19Document11 pagesSupplementary data and analyses for "Cardiovascular disease, drug therapy, and mortality in Covid-19hdjebarNo ratings yet
- Cameroon COVID AdherenceDocument6 pagesCameroon COVID AdherenceNfor LeonardNo ratings yet
- TabelDocument4 pagesTabelsatrianiNo ratings yet
- CINA Deluxe DQP Unknown DxConf For Brain Tumor Years 2012 2016 Updated 2-24-2020Document10 pagesCINA Deluxe DQP Unknown DxConf For Brain Tumor Years 2012 2016 Updated 2-24-2020MayNo ratings yet
- SML CML - FMFMDocument2 pagesSML CML - FMFMSaurabh MattaNo ratings yet
- Philippine Health DeliveryDocument89 pagesPhilippine Health Deliverysarguss14100% (5)
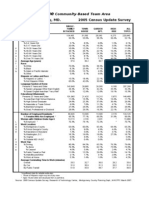
- Kemp Mill/Four Corners Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesKemp Mill/Four Corners Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Ações AtualDocument18 pagesAções Atualyatan001No ratings yet
- Georgia Avenue: Montgomery County, MD. 2005 Census Update SurveyDocument7 pagesGeorgia Avenue: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Culling and replacement rates in Canadian dairy herds from 2015-2020Document1 pageCulling and replacement rates in Canadian dairy herds from 2015-2020Ahmed KECHROUDNo ratings yet
- Culling and replacement rates in Canadian dairy herds from 2015-2020Document1 pageCulling and replacement rates in Canadian dairy herds from 2015-2020Ahmed KECHROUDNo ratings yet
- Genetics Cull eDocument1 pageGenetics Cull eAhmed KECHROUDNo ratings yet
- TB DotsDocument59 pagesTB Dotsreikomacky0% (1)
- 08 Chapter 08Document28 pages08 Chapter 08Miguel Antonio Barretto GarcíaNo ratings yet
- Normalized Balance SheetDocument1 pageNormalized Balance SheetPo_PimpNo ratings yet
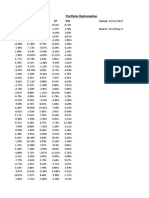
- Portfolio Optimization: BSRM Brac Beximco GP RAKDocument27 pagesPortfolio Optimization: BSRM Brac Beximco GP RAKFarsia Binte AlamNo ratings yet
- PharmaTrac Industry Mailer - Aug 2023Document8 pagesPharmaTrac Industry Mailer - Aug 2023LAKSHAY kUMARNo ratings yet
- NotesDocument1 pageNotesnahidhasan1981No ratings yet
- Osmani 2017 Final ReportDocument42 pagesOsmani 2017 Final Reportnahidhasan1981No ratings yet
- P10 Mixed Srategy PDFDocument10 pagesP10 Mixed Srategy PDFnahidhasan1981No ratings yet
- Lec 5Document38 pagesLec 5nahidhasan1981No ratings yet
- A File For ScribdDocument1 pageA File For Scribdnahidhasan1981No ratings yet
- Besley CoateDocument27 pagesBesley Coatenahidhasan1981No ratings yet
- 2016 QuestionnaireDocument45 pages2016 Questionnairenahidhasan1981No ratings yet
- PHD EconomicsDocument81 pagesPHD Economicsnahidhasan1981No ratings yet
- Obesity and Chronic DiseaseDocument63 pagesObesity and Chronic DiseaseNational Press FoundationNo ratings yet
- Lnfecciones Del Aparato Respiratorio SuperiorDocument23 pagesLnfecciones Del Aparato Respiratorio Superiormonterrubio_jl2909No ratings yet
- Concept Map 4 AnsiiDocument1 pageConcept Map 4 Ansiiapi-523409624No ratings yet
- NNCCS 2012Document27 pagesNNCCS 2012Nicole Louise N. VillanuevaNo ratings yet
- SR NO Time Specific Objective Content Teaching Learning Activity AV Aids EvaluationDocument22 pagesSR NO Time Specific Objective Content Teaching Learning Activity AV Aids EvaluationAkshata BansodeNo ratings yet
- An introduction to ethics in nursingDocument6 pagesAn introduction to ethics in nursingMohammad AzizNo ratings yet
- Ted Ed Nutrition VideosDocument2 pagesTed Ed Nutrition VideosMichael DunnNo ratings yet
- Curriculum VatieDocument2 pagesCurriculum VatienajammuftiNo ratings yet
- ET5740PTA 4430 (English)Document10 pagesET5740PTA 4430 (English)우승환Woo seung hwanNo ratings yet
- Person First Language Assignment Cook 1Document2 pagesPerson First Language Assignment Cook 1api-549604532No ratings yet
- Vaccinations in PregnancyDocument137 pagesVaccinations in PregnancyAmine YounisNo ratings yet
- Tuv 108.004 Iso 19011 2018Document2 pagesTuv 108.004 Iso 19011 2018Akshay Singh kushwahNo ratings yet
- KetoconazoleDocument2 pagesKetoconazoleMD. DELWAR HOSSAINNo ratings yet
- Holiday Hangover - Vocabulary - SDocument2 pagesHoliday Hangover - Vocabulary - SНастя КравченкоNo ratings yet
- Post Task For Module 2 Lessons 1 To 3: Give The Synthesis of The MovieDocument4 pagesPost Task For Module 2 Lessons 1 To 3: Give The Synthesis of The MoviePAM100% (1)
- ADHD and Your Teens: Behavior ManagementDocument1 pageADHD and Your Teens: Behavior ManagementKida7No ratings yet
- ArdsDocument69 pagesArdsdrabdallakawareNo ratings yet
- Dr. Oz Good Life - November 2015Document130 pagesDr. Oz Good Life - November 2015alejandronealNo ratings yet
- EPI Schedule of PakistanDocument1 pageEPI Schedule of Pakistanksbabar100% (1)
- Int Forum Allergy Rhinol - 2023 - Wise - International Consensus Statement On Allergy and Rhinology Allergic RhinitisDocument568 pagesInt Forum Allergy Rhinol - 2023 - Wise - International Consensus Statement On Allergy and Rhinology Allergic Rhinitishai1No ratings yet
- Health Care Delivery SystemDocument16 pagesHealth Care Delivery SystemUdaya Sree100% (4)
- A Systematic Review On Shifting Trends of Foodborne Diseases in PakistanDocument16 pagesA Systematic Review On Shifting Trends of Foodborne Diseases in PakistanAbasyn Journal of Life SciencesNo ratings yet
- 15 EO Oplan SitaDocument3 pages15 EO Oplan SitaSto Niño PagadianNo ratings yet
- SILVA METHOD The Five Rules For MindDocument5 pagesSILVA METHOD The Five Rules For MindVesna Radojevic100% (3)
- No Work No Pay Media Release - EnglishDocument3 pagesNo Work No Pay Media Release - EnglishJobar BuenaguaNo ratings yet
- Premium Shih Tzu Diet GuideDocument4 pagesPremium Shih Tzu Diet GuideJanet E. CariñoNo ratings yet
- Clare Gallagher - HSMS-An Analysis of System Types and EffectivenessDocument251 pagesClare Gallagher - HSMS-An Analysis of System Types and EffectivenessReza MuhammadNo ratings yet
- Normal Labour VIDEO + Module Final (5th June 2020)Document99 pagesNormal Labour VIDEO + Module Final (5th June 2020)Adam Chung100% (1)
- Safety LeadershipDocument38 pagesSafety LeadershipPrak Ba100% (2)
- The British High Commission Is An Equal Opportunity EmployerDocument4 pagesThe British High Commission Is An Equal Opportunity EmployerFahim John BhattiNo ratings yet