You might also like
- Review of Related LiteratureDocument28 pagesReview of Related LiteratureporseenaNo ratings yet
- Indonesian Older Adults Mental Health An OverviewDocument7 pagesIndonesian Older Adults Mental Health An OverviewSindy LarasatiNo ratings yet
- Sensory Processing Evaluation and Intervention in Mental Health - Mar10Document6 pagesSensory Processing Evaluation and Intervention in Mental Health - Mar10Kimberly WoodlandNo ratings yet
- Lesson 2B Implementation of Nursing Care of The Older Adult Psychosocial Care of Older AdultDocument6 pagesLesson 2B Implementation of Nursing Care of The Older Adult Psychosocial Care of Older Adultczeremar chanNo ratings yet
- Carren Maris N. Paculaba Cebu Normal University - College of Nursing Class 2013Document5 pagesCarren Maris N. Paculaba Cebu Normal University - College of Nursing Class 2013carrenmaris_48No ratings yet
- 2.dipty SubbaDocument12 pages2.dipty SubbaAnonymous CwJeBCAXpNo ratings yet
- 213 FullDocument9 pages213 Fullapi-239715101No ratings yet
- McKee Lynzie FinalDocument34 pagesMcKee Lynzie FinalverdadolarevicNo ratings yet
- Liran Rafaely, Sara Carmel & Yaacov G. Bachner (2018)Document9 pagesLiran Rafaely, Sara Carmel & Yaacov G. Bachner (2018)vascoNo ratings yet
- Stress and The Biopsychosocial Model in Middle and Late AdulthoodDocument14 pagesStress and The Biopsychosocial Model in Middle and Late AdulthoodE-libraryNo ratings yet
- 1 s2.0 S0883941711001294 Main PDFDocument11 pages1 s2.0 S0883941711001294 Main PDFMarlowe SarabiaNo ratings yet
- The Influence of Resilience On Psychological Distress in University StudentsDocument6 pagesThe Influence of Resilience On Psychological Distress in University StudentsDeahNo ratings yet
- Chapter 2Document7 pagesChapter 2Christine Mae Viñas RemoNo ratings yet
- Stress On Health-Related Quality of Life in Older Adults The Protective Nature of MindfulnessDocument7 pagesStress On Health-Related Quality of Life in Older Adults The Protective Nature of MindfulnessChhavi MudgalNo ratings yet
- The Austerity Cure: The Impact of Benefit Sanctions on Mental HealthFrom EverandThe Austerity Cure: The Impact of Benefit Sanctions on Mental HealthNo ratings yet
- Effects of Mindfulness-Based Interventions On Self-Compassion in Health Care Professionals: A Meta-AnalysisDocument21 pagesEffects of Mindfulness-Based Interventions On Self-Compassion in Health Care Professionals: A Meta-AnalysisEstigma Universidad Del RosarioNo ratings yet
- Salome PDocument13 pagesSalome PJames MwabwalwaNo ratings yet
- Psychometric Evaluation of The Financial Threat Scale (FTS) in The Context of The Great RecessionDocument10 pagesPsychometric Evaluation of The Financial Threat Scale (FTS) in The Context of The Great RecessionJeffery McDonaldNo ratings yet
- Health Psychology AssignmentDocument9 pagesHealth Psychology AssignmentmariaNo ratings yet
- Kalket and Wilson-Milestone 3 Literature ReviewDocument13 pagesKalket and Wilson-Milestone 3 Literature Reviewapi-704711481No ratings yet
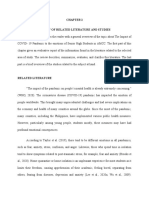
- Review of Related Literature and StudiesDocument3 pagesReview of Related Literature and StudiesValerie Ann EscobarNo ratings yet
- s0156958 Monica-Leigh Reitano Hlth2029Document5 pagess0156958 Monica-Leigh Reitano Hlth2029moccie123No ratings yet
- Tigma and ORK: Heather StuartDocument12 pagesTigma and ORK: Heather StuartRatu Nurul AfiniNo ratings yet
- A1 The Effect of Environmental Factors and Social Circumtances To Mental Health OCADocument7 pagesA1 The Effect of Environmental Factors and Social Circumtances To Mental Health OCAB1. Rosalinda Angelika PutriNo ratings yet
- Mental Health AssignmentDocument7 pagesMental Health AssignmentOlofin SamuelNo ratings yet
- Final Resilience-5Document18 pagesFinal Resilience-5api-707377790No ratings yet
- Research PaperDocument8 pagesResearch PaperJamaica LoberianoNo ratings yet
- 3910 Understanding Social Research Mental Health Portfolio Assignment 2 - 3 2Document27 pages3910 Understanding Social Research Mental Health Portfolio Assignment 2 - 3 2api-628734736No ratings yet
- Acp 10 039Document11 pagesAcp 10 039Marta Castillo FalcónNo ratings yet
- Chapter Three Identification and Differentiated Services: Learning OutcomesDocument68 pagesChapter Three Identification and Differentiated Services: Learning OutcomesdawitNo ratings yet
- Zeeshan and AslamDocument11 pagesZeeshan and AslamDian Atnantomi WiliyantoNo ratings yet
- Mentus, Vladimir S. - Determinante Mentalnog Blagostanja U Srbiji (Clanak)Document26 pagesMentus, Vladimir S. - Determinante Mentalnog Blagostanja U Srbiji (Clanak)Ed BlackadderNo ratings yet
- DPB A1 SampleDocument11 pagesDPB A1 SampleE-libraryNo ratings yet
- I. Background/Objectives and GoalsDocument2 pagesI. Background/Objectives and GoalsJilmilyn MolenoNo ratings yet
- Do Big Five Personality Traits Moderate The Effects ofDocument12 pagesDo Big Five Personality Traits Moderate The Effects ofKa Wing LeungNo ratings yet
- Stress Among College Students FileDocument59 pagesStress Among College Students FileTushar KapoorNo ratings yet
- Diathesis-Stress and PWBDocument6 pagesDiathesis-Stress and PWBMuhammad AminullahNo ratings yet
- Universiti Malaysia Sarawak Faculty of Built Environment Faculty of EngineeringDocument6 pagesUniversiti Malaysia Sarawak Faculty of Built Environment Faculty of EngineeringAnselm TawNo ratings yet
- Mental HealthDocument16 pagesMental HealthYessa CaesarNo ratings yet
- Final Thesis BindingDocument49 pagesFinal Thesis BindingMuskanNo ratings yet
- Population Health EssayDocument3 pagesPopulation Health Essaybrooke hootonNo ratings yet
- 100 904 2 PBDocument15 pages100 904 2 PBRizka AnggiaNo ratings yet
- Exploring Anxiety and Academic Performance Among University Students in UAEDocument18 pagesExploring Anxiety and Academic Performance Among University Students in UAEWaseel sultanNo ratings yet
- Final Research PaperDocument17 pagesFinal Research Paperapi-451460387No ratings yet
- Emotion Focused Therapy For Generalized Anxiety Intro SampleDocument14 pagesEmotion Focused Therapy For Generalized Anxiety Intro SamplemoizNo ratings yet
- Neurocognitive Impairment Addressing Couple and Family ChallengesDocument20 pagesNeurocognitive Impairment Addressing Couple and Family ChallengesFrancisca Cid BelmarNo ratings yet
- Profiles of Resilience and Psychosocial Outcomes Among Young Black Gay and Bisexual MenDocument17 pagesProfiles of Resilience and Psychosocial Outcomes Among Young Black Gay and Bisexual MenFirmanNo ratings yet
- Effect of Childhood Psychological TraumaDocument23 pagesEffect of Childhood Psychological TraumaSea SaltNo ratings yet
- 1-s2 0-S0021992405000213-MainDocument25 pages1-s2 0-S0021992405000213-Mainapi-253276589No ratings yet
- Project SynopsisDocument11 pagesProject SynopsisManoshi SharmaNo ratings yet
- Ijpher: Research ArticleDocument9 pagesIjpher: Research ArticlePremier PublishersNo ratings yet
- Fnbeh 08 00241 PDFDocument14 pagesFnbeh 08 00241 PDFymintriagoNo ratings yet
- 1 s2.0 S0191886922004573 MainDocument12 pages1 s2.0 S0191886922004573 Mainreza.scienceloverNo ratings yet
- Experiences of Dynamic Bullying VictimsDocument19 pagesExperiences of Dynamic Bullying VictimsVaishnavi VisnuNo ratings yet
- ZawadzskiDocument11 pagesZawadzskiapi-340134451No ratings yet
- Differences in Cognitive Performance Between Informal Caregivers and Non-CaregiversDocument25 pagesDifferences in Cognitive Performance Between Informal Caregivers and Non-CaregiversIshani SharmaNo ratings yet
- Thesis 1st DraftDocument99 pagesThesis 1st DraftcampaignwhoNo ratings yet
- Stress and Worry: Examining Intolerance of Uncertainty 'S Moderating EffectDocument14 pagesStress and Worry: Examining Intolerance of Uncertainty 'S Moderating EffectsolleeyNo ratings yet
- ROL Empty Chair 2Document22 pagesROL Empty Chair 2tbf06720No ratings yet
- Hepran2017 159 167Document9 pagesHepran2017 159 167Elizabethan VictoriaNo ratings yet
- A Study On Health and Safety Measures of Chemical Industries With Reference To Palakkad RegionDocument60 pagesA Study On Health and Safety Measures of Chemical Industries With Reference To Palakkad Regionporseena0% (1)
- Warehousing Functions and TypesDocument5 pagesWarehousing Functions and TypesporseenaNo ratings yet
- Factors You Consider While Opening A New AccountDocument4 pagesFactors You Consider While Opening A New AccountporseenaNo ratings yet
- Factors Affecting The Efficiency in Warehouse Management of Supermarkets in NairobiDocument1 pageFactors Affecting The Efficiency in Warehouse Management of Supermarkets in NairobiporseenaNo ratings yet
- Inaugural Session: 9.30 - 10.45 A.m: Smt. Sumathi KrishnaprasadDocument1 pageInaugural Session: 9.30 - 10.45 A.m: Smt. Sumathi KrishnaprasadporseenaNo ratings yet
- 7212, Karpagam Institute of Technology Coimbatore - 641 105 Department of Management Studies Absentees StatementDocument2 pages7212, Karpagam Institute of Technology Coimbatore - 641 105 Department of Management Studies Absentees StatementporseenaNo ratings yet
- Math Probes I (B) - II STDDocument8 pagesMath Probes I (B) - II STDporseenaNo ratings yet
- Principles of Effective CommunicationDocument7 pagesPrinciples of Effective Communicationporseena100% (3)
- BA 7051 Logistics and Supply Chain Management UNIT - 1Document13 pagesBA 7051 Logistics and Supply Chain Management UNIT - 1porseenaNo ratings yet
- Unit - 4 (MC)Document22 pagesUnit - 4 (MC)porseenaNo ratings yet
- OB Response: Global and Cultural DiversityDocument9 pagesOB Response: Global and Cultural DiversityporseenaNo ratings yet
- Group DynamicsDocument25 pagesGroup DynamicsporseenaNo ratings yet
- Forms Ofbusiness OrganizationDocument21 pagesForms Ofbusiness OrganizationporseenaNo ratings yet
- Victim or Survivor TerminologyDocument2 pagesVictim or Survivor TerminologyRohit James JosephNo ratings yet
- Alcohol ConcentrationDocument5 pagesAlcohol Concentrationapi-299736788No ratings yet
- Test Bank For Child Maltreatment An Introduction 3rd Edition Cindy L Miller PerrinDocument7 pagesTest Bank For Child Maltreatment An Introduction 3rd Edition Cindy L Miller PerrinScott Romero100% (32)
- Speech About BullyingDocument1 pageSpeech About BullyingBaby Let Alaban100% (1)
- CSEC Caribbean History June 2015 P2Document24 pagesCSEC Caribbean History June 2015 P2Sachin Bahadoorsingh100% (2)
- Zimpli Kids LTD Labour and Ethics PolicyDocument7 pagesZimpli Kids LTD Labour and Ethics PolicyZimpli KidsNo ratings yet
- Assessing ViolenceDocument6 pagesAssessing ViolenceKarlo Jose Dao-ayanNo ratings yet
- Anti-Violence Against Women and Children (Vawc)Document80 pagesAnti-Violence Against Women and Children (Vawc)Chin Martinz100% (3)
- Scapegoat - Andrea Dworkin PDFDocument446 pagesScapegoat - Andrea Dworkin PDFMaria Del Carmen Chavez Lamas100% (1)
- Davies, J.M. (1998) - Between The Disclosure and Foreclosure of Erotic Transference-CountertransferenceDocument12 pagesDavies, J.M. (1998) - Between The Disclosure and Foreclosure of Erotic Transference-CountertransferencemajaninNo ratings yet
- Rebuttal EssayDocument3 pagesRebuttal EssayBob CrossNo ratings yet
- 5 Emerging Issues On FamiliesDocument57 pages5 Emerging Issues On Familieslyka100% (2)
- Davao City LesbianDocument3 pagesDavao City LesbianMau MerlNo ratings yet
- Classic-Newspaper-211 AutorecoverDocument5 pagesClassic-Newspaper-211 Autorecoverapi-666660222No ratings yet
- Child Slavery: Read The Following Article, and Then Answer The Questions That FollowDocument4 pagesChild Slavery: Read The Following Article, and Then Answer The Questions That FollowManal SalNo ratings yet
- L 4a Signs and SymptomsDocument27 pagesL 4a Signs and SymptomsSemeeeJuniorNo ratings yet
- Faculty LetterDocument2 pagesFaculty LetterMLive.comNo ratings yet
- Kincaid. Child-Loving PDFDocument427 pagesKincaid. Child-Loving PDFSebastián50% (4)
- Chapter 16T - America's Drug Lords, Banksters, & War CriminalsDocument34 pagesChapter 16T - America's Drug Lords, Banksters, & War CriminalsGTX357-Bruce Gorcyca Book ManuscriptsNo ratings yet
- Child Labor SpeechDocument2 pagesChild Labor SpeechVania0% (1)
- Attorneys For Defendants Gary R. Herbert and John E. SwallowDocument13 pagesAttorneys For Defendants Gary R. Herbert and John E. SwallowEquality Case FilesNo ratings yet
- E-C-Q-, AXXX XXX 146 (BIA Nov. 17, 2017)Document24 pagesE-C-Q-, AXXX XXX 146 (BIA Nov. 17, 2017)Immigrant & Refugee Appellate Center, LLC0% (1)
- PTSD TrainingDocument32 pagesPTSD TrainingThe Institute for Innovation & ImplementationNo ratings yet
- Bongalon vs. PeopleDocument13 pagesBongalon vs. PeopleJoan Eunise FernandezNo ratings yet
- Gender Profile of The Philippines: Group ADocument19 pagesGender Profile of The Philippines: Group AMike Zach Acebedo Abarsosa100% (1)
- Winning StrategiesDocument43 pagesWinning StrategiesDestiny Ann100% (5)
- Sarah Kane Crave PDFDocument27 pagesSarah Kane Crave PDFGuilherme ZiebellNo ratings yet
- BBB Vs AAA GR No. 193225Document10 pagesBBB Vs AAA GR No. 193225diamajolu gaygonsNo ratings yet
- Script For GSPSDocument10 pagesScript For GSPSjamaica caseresNo ratings yet
- Purposive CommunicationDocument4 pagesPurposive CommunicationMadriñan Wency M.No ratings yet