You might also like
- Clinical Efficacy of Azithromycin Versus Co-Amoxiclave in Acute Otitis MediaDocument7 pagesClinical Efficacy of Azithromycin Versus Co-Amoxiclave in Acute Otitis MediaAndry YonathaNo ratings yet
- Physical Activity QuestionnaireDocument4 pagesPhysical Activity QuestionnaireAndry YonathaNo ratings yet
- Nutrition in Emergencies: Types, Definitions, StrategiesDocument9 pagesNutrition in Emergencies: Types, Definitions, StrategiesAndry YonathaNo ratings yet
- Malnutrition: Protein / EnergyDocument26 pagesMalnutrition: Protein / EnergyAndry YonathaNo ratings yet
- Ciri-Ciri Sindroma DownDocument5 pagesCiri-Ciri Sindroma DownAndry YonathaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Output Configurations and Connections: NPN Open CollectorDocument2 pagesOutput Configurations and Connections: NPN Open Collectordorin serbanNo ratings yet
- Ajhgaa English O6Document28 pagesAjhgaa English O6dhirumeshkumarNo ratings yet
- D-Glucitol (420i) Dextrose MonohydrateDocument3 pagesD-Glucitol (420i) Dextrose MonohydrateSilvia Melendez HNo ratings yet
- Presentation 1Document26 pagesPresentation 1Vaibhav Hireraddi100% (1)
- Casa Cook ArvindDocument65 pagesCasa Cook ArvindLEAN MauritiusNo ratings yet
- Portland Traffic Crash Report 2021Document11 pagesPortland Traffic Crash Report 2021KGW NewsNo ratings yet
- Captain Marvel (DC Comics) : Shazam! Navigation SearchDocument34 pagesCaptain Marvel (DC Comics) : Shazam! Navigation SearchAce Orense Cupid Uranus Ace Sphinx Galzu Acetr444 son of Multiverses Chaos Gaeia Eros ACETR444No ratings yet
- TDS - RheoFIT 762Document2 pagesTDS - RheoFIT 762Alexi ALfred H. TagoNo ratings yet
- 405 Econometrics Odar N. Gujarati: Prof. M. El-SakkaDocument27 pages405 Econometrics Odar N. Gujarati: Prof. M. El-SakkaKashif KhurshidNo ratings yet
- Creative NonfictionDocument11 pagesCreative NonfictionRubelyn CagapeNo ratings yet
- Premchand Deliverance Download in PDFDocument4 pagesPremchand Deliverance Download in PDFRiya W100% (3)
- Wattgate 381 Audio Grade Duplex Socket - y CableDocument20 pagesWattgate 381 Audio Grade Duplex Socket - y Cableapi-11530725100% (1)
- Surface-Based Transport Model For Mixed-Size Sediment: Peter R. Wilcock, M.ASCE, and Joanna C. CroweDocument9 pagesSurface-Based Transport Model For Mixed-Size Sediment: Peter R. Wilcock, M.ASCE, and Joanna C. CroweEdwinNo ratings yet
- Satellite Communication Uplink Transmitter Downlink Receiver and TransponderDocument2 pagesSatellite Communication Uplink Transmitter Downlink Receiver and TransponderTHONTARADYA CHANNELNo ratings yet
- Papaya Burger - Chapter 1 6Document129 pagesPapaya Burger - Chapter 1 6Nicole Velasco NuquiNo ratings yet
- Product Information: Traffic Management AccessoryDocument12 pagesProduct Information: Traffic Management AccessoryCORAL ALONSONo ratings yet
- Caffeine Extraction 1 PDFDocument25 pagesCaffeine Extraction 1 PDFShanay ShahNo ratings yet
- B. WoolworthsDocument5 pagesB. WoolworthsNjabulo Shakes NtuliNo ratings yet
- GRT9165 Product GuideDocument23 pagesGRT9165 Product GuideEslamAldenAbdoNo ratings yet
- Electric Charge: Conservation and Quantization Conductors, Insulators, and Induced ChargesDocument21 pagesElectric Charge: Conservation and Quantization Conductors, Insulators, and Induced ChargesAcadGucciManeNo ratings yet
- Word Trek Lesson OutlinesDocument8 pagesWord Trek Lesson Outlinesapi-289048378No ratings yet
- SmogDocument5 pagesSmogAlain MoratallaNo ratings yet
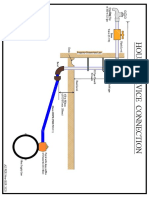
- House Service Connection NEW BSR 2020-1Document1 pageHouse Service Connection NEW BSR 2020-1Deshraj BairwaNo ratings yet
- Assignment IDocument2 pagesAssignment Ivaishnavi priyaNo ratings yet
- Elcometer Wet-Film Gage 115 Spec SheetDocument2 pagesElcometer Wet-Film Gage 115 Spec SheetMary CasillasNo ratings yet
- NPC PrintPlay DeckDocument19 pagesNPC PrintPlay DeckBenjamin Pappa Bach FossumNo ratings yet
- Chips Unlimited Blend LibraryDocument20 pagesChips Unlimited Blend Librarymizan sallehNo ratings yet
- Transmission Lines Explained for Efficiency and Loss ReductionDocument25 pagesTransmission Lines Explained for Efficiency and Loss Reductionjagdish choudharyNo ratings yet
- RepairManual NEF M100 M150 P3D32N003E Mar06Document172 pagesRepairManual NEF M100 M150 P3D32N003E Mar06manuel segovia100% (1)
- Potensi Energi Listrik Yang Dihasilkan Dari Emisi Gas Metana Di Tpa Suwung Provinsi BaliDocument8 pagesPotensi Energi Listrik Yang Dihasilkan Dari Emisi Gas Metana Di Tpa Suwung Provinsi BaliNuyul FaizahNo ratings yet