You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- English Vocabulary: No. Nama FotoDocument7 pagesEnglish Vocabulary: No. Nama Fotofiora.ladesvitaNo ratings yet
- English Vocabulary 2: No. Nama FotoDocument8 pagesEnglish Vocabulary 2: No. Nama Fotofiora.ladesvitaNo ratings yet
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyDocument10 pagesDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaNo ratings yet
- Quat Trin 2006Document10 pagesQuat Trin 2006fiora.ladesvitaNo ratings yet
- Mahjoob2014 PDFDocument5 pagesMahjoob2014 PDFfiora.ladesvitaNo ratings yet
- Eilers 2007Document12 pagesEilers 2007fiora.ladesvitaNo ratings yet
- Des An Jose 2019Document6 pagesDes An Jose 2019fiora.ladesvitaNo ratings yet
- Vocab Coco 2Document7 pagesVocab Coco 2fiora.ladesvitaNo ratings yet
- Smooth Sailing - Navigating The Sea of Law Applicable To The CruiDocument35 pagesSmooth Sailing - Navigating The Sea of Law Applicable To The Cruifiora.ladesvitaNo ratings yet
- 1St Floor: House On Paus Schematic Plan ProgressDocument2 pages1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaNo ratings yet
- F374W1M2L5G52563 FirstDocument1 pageF374W1M2L5G52563 Firstfiora.ladesvitaNo ratings yet
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocument12 pagesChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaNo ratings yet
- Gibson 2010Document19 pagesGibson 2010fiora.ladesvitaNo ratings yet
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyDocument11 pagesSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaNo ratings yet
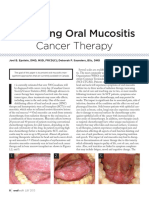
- Managing Oral Mucositis Oral Health July 2015Document4 pagesManaging Oral Mucositis Oral Health July 2015fiora.ladesvitaNo ratings yet
- Abdul Kadir 2016Document7 pagesAbdul Kadir 2016fiora.ladesvitaNo ratings yet
- Lalla 2008Document17 pagesLalla 2008fiora.ladesvitaNo ratings yet
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocument12 pagesChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaNo ratings yet
- Quat Trin 2006Document10 pagesQuat Trin 2006fiora.ladesvitaNo ratings yet
- Full TextDocument127 pagesFull Textfiora.ladesvitaNo ratings yet
- G15 v03 ED Design Guidelines Dec-14Document77 pagesG15 v03 ED Design Guidelines Dec-14gracegozaliNo ratings yet
- ID Perbandingan Kualitas Hidup Pasien Gagal PDFDocument9 pagesID Perbandingan Kualitas Hidup Pasien Gagal PDFAlawiyahRasyaNo ratings yet
- Ambulatory Care Nursing: Coming Soon!Document16 pagesAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaNo ratings yet
- Lalla 2008Document17 pagesLalla 2008fiora.ladesvitaNo ratings yet
- 2015 Conference 10Document11 pages2015 Conference 10fiora.ladesvitaNo ratings yet
- Anderson2004 PDFDocument7 pagesAnderson2004 PDFfiora.ladesvitaNo ratings yet
- Medicalscience: EcancerDocument7 pagesMedicalscience: Ecancerfiora.ladesvitaNo ratings yet
- Assessment Rating ScaleDocument8 pagesAssessment Rating Scalefiora.ladesvitaNo ratings yet
- Ni Hms 544150Document15 pagesNi Hms 544150fiora.ladesvitaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 5 Stages of Grief and Acceptance ProcessDocument19 pages5 Stages of Grief and Acceptance ProcessWendy Veeh Tragico BatarNo ratings yet
- Bible Verses 19 & 20Document1 pageBible Verses 19 & 20RoomMomExtraNo ratings yet
- The Secrets To Charisma and Personal Magnetism - Learn A Hidden Energy Tradition To Become Magnetically Attractive and Vitally Alive (Personal Magnetism Series Book 1)Document117 pagesThe Secrets To Charisma and Personal Magnetism - Learn A Hidden Energy Tradition To Become Magnetically Attractive and Vitally Alive (Personal Magnetism Series Book 1)Hendro Santoso82% (11)
- Narag V NaragDocument18 pagesNarag V NaragMp CasNo ratings yet
- " Wendy - B. Howard.: Despatch Magazine Vol. 26:1 Nov., 2014Document100 pages" Wendy - B. Howard.: Despatch Magazine Vol. 26:1 Nov., 2014sterhowardNo ratings yet
- RMY 101 Assignment Fall 2020 InstructionsDocument5 pagesRMY 101 Assignment Fall 2020 InstructionsAbass GblaNo ratings yet
- 100 Thai BooksDocument7 pages100 Thai BooksJizelle M. AuditorNo ratings yet
- In 1947 A Corps of Architects and Engineers Were Tasked To Study The Modern US and Latin American Capitals and Formulate A Master Plan For ManilaDocument7 pagesIn 1947 A Corps of Architects and Engineers Were Tasked To Study The Modern US and Latin American Capitals and Formulate A Master Plan For ManilaEliza Mae AquinoNo ratings yet
- Syllabus YTE Version0.2Document10 pagesSyllabus YTE Version0.2Sam MeshramNo ratings yet
- Dimitrios A. Vasilakis Hellenism and Christianity Petros Vrailas-Armenis On The Constituents of Modern Greek IdentityDocument21 pagesDimitrios A. Vasilakis Hellenism and Christianity Petros Vrailas-Armenis On The Constituents of Modern Greek IdentityPanagiotis AndriopoulosNo ratings yet
- 118 - Throwing in The TowelDocument2 pages118 - Throwing in The TowelDavid E RobinsonNo ratings yet
- Secularism in India (Sitaram Goel)Document32 pagesSecularism in India (Sitaram Goel)Ramesh RamaNo ratings yet
- JONES - Blues People - Negro Music in White AmericaDocument46 pagesJONES - Blues People - Negro Music in White AmericaNatalia ZambaglioniNo ratings yet
- Guru Granth Sahib Little Taste PDFDocument12 pagesGuru Granth Sahib Little Taste PDFG SNo ratings yet
- Helen of TroyDocument2 pagesHelen of TroyPatrick FranciaNo ratings yet
- The Reality of HellDocument7 pagesThe Reality of HellThe Fatima CenterNo ratings yet
- (English) ENGLISH SPEECH - DONALD TRUMP - Never, Ever Give Up (English Subtitles)Document16 pages(English) ENGLISH SPEECH - DONALD TRUMP - Never, Ever Give Up (English Subtitles)Huan NguyenNo ratings yet
- Learning about the Sixth CommandmentDocument20 pagesLearning about the Sixth CommandmentΑδελφοσ ΝονNo ratings yet
- Role of Whistling in Peruvian Ayahuasca HealingDocument9 pagesRole of Whistling in Peruvian Ayahuasca HealingjuiceshakeNo ratings yet
- U2 Science Theology Copernican Revolution 12pages 2012-8-13Document6 pagesU2 Science Theology Copernican Revolution 12pages 2012-8-13James JiangNo ratings yet
- Liber GomorrhianusDocument95 pagesLiber GomorrhianusMaxi AguaysolNo ratings yet
- Self Existence of God Dr. Venkat PotanaDocument3 pagesSelf Existence of God Dr. Venkat PotanaDr. Potana Venkateswara RaoNo ratings yet
- Continental Monthly:: Literature and National PolicyDocument127 pagesContinental Monthly:: Literature and National PolicyGutenberg.orgNo ratings yet
- When God Was BlackDocument102 pagesWhen God Was BlackJesse FaulknerNo ratings yet
- Imam Ghazali's Influence on Islamic PsychologyDocument2 pagesImam Ghazali's Influence on Islamic Psychologyfaizafazal.900100% (1)
- Architecture As A Manifest of The Culture of A Region: Cite This PaperDocument13 pagesArchitecture As A Manifest of The Culture of A Region: Cite This PaperakshayaNo ratings yet
- AkashaDocument106 pagesAkashacrysty cristy100% (4)
- The Western CanonDocument42 pagesThe Western CanonLiviu SNo ratings yet
- Book Review Gods in Early BuddhismDocument1 pageBook Review Gods in Early BuddhismmahiyagiNo ratings yet
- Chronological Overview of Architecture-CompressedDocument139 pagesChronological Overview of Architecture-CompressedzarinaNo ratings yet