Professional Documents
Culture Documents
Balam I 2012 Compli Hip
Uploaded by
Rosario RosarioOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Balam I 2012 Compli Hip
Uploaded by
Rosario RosarioCopyright:
Available Formats
Review
Complications of intracerebral haemorrhage
Joyce S Balami, Alastair M Buchan
Intracerebral haemorrhage (ICH) is the most devastating type of stroke and is a leading cause of disability and mortality. Lancet Neurol 2012; 11: 101–18
By contrast with advances in ischaemic stroke treatment, few evidence-based targeted treatments exist for ICH. Acute Stroke Programme,
Management of ICH is largely supportive, with strategies aimed at the limitation of further brain injury and the Department of Medicine and
Clinical Geratology
prevention of associated complications, which add further detrimental effects to an already lethal disease and jeopardise (J S Balami MRCP), and Acute
clinical outcomes. Complications of ICH include haematoma expansion, perihaematomal oedema with increased Vascular Imaging Centre,
intracranial pressure, intraventricular extension of haemorrhage with hydrocephalus, seizures, venous thrombotic University of Oxford
events, hyperglycaemia, increased blood pressure, fever, and infections. In view of the restricted number of therapeutic (Prof A M Buchan FMedSci),
Oxford University Hospitals
options for patients with ICH, improved surveillance is needed for the prevention of these complications, or, when this NHS Trust, Oxford, UK
is not possible, early detection and optimum management, which could be effective in the reduction of adverse effects Correspondence to:
early in the course of stroke and in the improvement of prognosis. Further studies are needed to enhance the evidence- Prof Alastair M Buchan,
based recommendations for the management of this important clinical problem. Biomedical Research Centre,
University of Oxford, Oxford
University Hospitals NHS
Introduction treatment for ICH, and whether or not surgical Trust, John Radcliffe,
Spontaneous or primary intracerebral haemorrhage approaches are beneficial remains controversial. Oxford, OX3 9DU, UK
(ICH) is a major cause of morbidity and mortality Additional therapeutic dilemmas can arise over the alastair.buchan@medsci.ox.
worldwide. It is the second most common form of stroke, safest and most effective approach to VTE prevention in ac.uk
accounting for 10–30% of first-ever strokes.1–3 The 30 day patients with ICH because prophylaxis with anti-
mortality for ICH has been reported to be 30–55%,1–6 with coagulants can increase the risk of HE or further
half the deaths occurring in the acute phase, especially in bleeding. Perhaps a more difficult therapeutic dilemma
the first 48 h.1,2,5 The complications of ICH are among the is how to manage patients with clinical thromboembolic
major predictors of early mortality and poor outcome. complications after ICH, balancing the risk of subsequent
ICH complications include haematoma expansion life-threatening thromboembolism if untreated against
(HE), perihaematomal oedema (PHE), intraventricular the risk of recurrence of ICH. A related issue is whether
extension of haemorrhage (IVH) with hydrocephalus, or when to resume anticoagulation after ICH in patients
seizures, venous thromboembolic events (VTE), hyper- with cardiac disease associated with high embolism risk,
glycaemia, increased blood pressure (BP), fever, and such as those who need mechanical valve prostheses or
infections. Complications such as HE,7,8 IVH with those with atrial fibrillation.
obstructive hydrocephalus,9–11 and hyperglycaemia4,12,13 In this review, we focus on the early complications of
are major predictors of increased early mortality and ICH, discussing emerging therapies and relevant
adverse outcome during the hyperacute phase of ICH. preventative and management strategies based on
Similarly, HE, hydrocephalus, and PHE have been available evidence and guidelines. We draw attention to
associated with early neurological deterioration (END) the scarcity of evidence to guide the management of
and poor outcome.14 A prospective observational study many important and common complications of ICH.
reported END in about 33% of patients with ICH within
48 h of onset, with an associated 30 day mortality of 47% Haematoma expansion
in those with END.14 Clinical features
The complications of ischaemic stroke (IS) and their HE, defined as an increase in volume of 33–50% or an
management have been reviewed extensively,15,16 with absolute change in haematoma volume of 12·5–20 mL
little discussion of the complications of ICH. Despite its (on repeat CT), is a common early and severe complication
seriousness, the treatment options for ICH are restricted of ICH.8,17–20 Although HE is one of the main pathophysio-
and few evidence-based data exist to guide the logical phases of ICH, it can also be a serious complication
management of ICH complications. By contrast with IS, subsequent to the acute phase—up to 40% of the
for which therapeutic advances have been made to haematoma grows in the first few hours post ictus.
improve clinical outcome, the management of ICH is Various terms such as haematoma extension, expansion,
generally supportive, but with poor prognosis because no progression, growth, enlargement, and rebleeding have
specific treatments have been shown to improve outcome been used to describe this subsequent increase in
after ICH. For example, the management of HE is of haematoma volume after ICH.
unproven value because all measures aimed at restricting The precise mechanism of early HE during the acute
HE have so far not improved outcome in controlled trials. phase is poorly understood. It is proposed to be a
Similarly, PHE management is mainly supportive and heterogeneous process that includes dysregulation of
measures aimed at decreasing intracranial pressure haemostasis via inflammatory cascade activation and
(ICP) are also of unproven value. Also, insufficient matrix metalloproteinase (MMP) overexpression, break-
evidence exists with regard to the efficacy of surgical down of the blood–brain barrier, a sudden increase in
www.thelancet.com/neurology Vol 11 January 2012 101
Review
A B C D
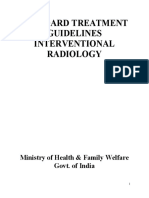
Figure 1: CT angiogram showing contrast extravasation
Arrowheads indicate contrast extravasation. Spot-sign score 1 (A), 2 (B), 3(C), and 4 (D). Reproduced from Delgado Almandoz and colleagues,31 by permission of
Wolters Kluwer Health.
ICP leading to local tissue distortion and disruption, and Other important predictors of HE include large
vascular engorgement due to reduced venous outflow.8 haematoma volume on presentation,29,32 early presentation
Early HE can also result from an increased plasma (especially within 3 h of onset),17,19,29,32 heterogeneity of
concentration of cellular fibronectin (c-FN) and the in- haematoma density on admission CT,33 and prior use of
flammatory mediator interleukin-6 (IL-6).21 Pathological warfarin.17,24,25 Blood biomarkers such as increased IL-6,
studies have shown multiple microscopic and macro- MMP-9, c-FN, and tumour necrosis factor, reduced
scopic bleeding points around the border of platelet activity,21 reduced fibrinogen concentrations,19
haemorrhages, arising from ruptured arterioles or and increased serum creatinine,32 have been suggested to
venules that result from the stretching of surrounding predict HE in patients with ICH. Conflicting results were
vessels after clot expansion.22 seen for increased D-dimers as a predictor of HE.34,35
Several studies indicate that early HE occurs in 18–38% Some studies have shown an association between systolic
of patients scanned within 3 h of ICH onset7,18,19 and more BP (SBP) and HE,36,37 but others have not.7,19,32,38 Similarly,
than 70% develop at least some extent of HE within 24 h some studies show an association between prior use of
of symptom onset,23 even in the absence of known antiplatelet drugs and HE,32,34,39 although others do not.40,41
coagulopathy, suggesting an active bleeding process in Other risk factors include hyperglycaemia,4,12,36 previous
the hyperacute phase of ICH.22 In warfarin-associated cerebral infarction, liver disease,36 a decreased level of
ICH, 27–54% of patients develop early HE and a delayed consciousness, and heavy alcohol intake.19
expansion because of protracted bleeding,24–26 which is HE is often associated with END and is an independent
associated with up to 70% increase in mortality.24,27 predictor of poor outcome and increased mortality.1,8,23,42
A prospective study showed 38% of patients had an Findings from a meta-analysis of 218 patients with ICH
increase in haematoma volume (>33% increase compared who had CT scans within 3 h of onset and follow-up
with admission CT) within 3 h of symptom onset. HE scans within 24 h23 showed that for every 10% increase in
was evident even within 1 h of the baseline scan in two- ICH growth there was a 5% increased risk of death, a
thirds of those patients, whereas an additional 12% 16% increased risk of worsening outcome as measured
developed growth within the next 21 h, which suggests with the modified Rankin score (mRS), and an 18%
continued active bleeding.7 Subsequent prospective increased likelihood of being dependent or of a poor
studies have confirmed this finding, noting that 23–32% outcome on the Barthel index.
of patients had an increase in haematoma volume (>33%
from baseline or 12·5 mL) in the first 24 h.8,20 Management
CT angiographic studies that show contrast extra- Interventions to restrict HE include haemostatic
vasation (the so-called spot sign) into the haematoma28–30 therapy, cautious lowering of high BP, quick reversal of
have provided additional evidence of progressive bleeding prior anticoagulation, and surgical evacuation (table 1).
several hours after the onset of ICH. The spot sign is an Clinical trials8,43 targeting HE in ICH and a meta-
important predictor of haematoma growth and might be analysis65 have shown that the use of recombinant factor
useful in the prediction of HE with high specificity28–30 VII (rFVIIa) limits the extent of HE in patients with
and as a predictor of mortality.28,30,31 In fact, the spot-sign non-coagulopathic ICH. However, there was an increase
score (figure 1), which is used to grade the number of in thromboembolic risk with no clear clinical benefit in
spot signs and their maximum dimensions and unselected patients. The SPOTLIGHT (Spot Sign
attenuation, is the strongest predictor of HE and is an Selection of Intracerebral Hemorrhage to Guide
independent predictor of in-hospital mortality and poor Hemostatic Therapy; ClinicalTrials.gov identifier
outcome in people with ICH.31 NCT01359202) and STOP-IT (Spot Sign for Predicting
102 www.thelancet.com/neurology Vol 11 January 2012
Review
Description Level of
evidence*
Medical management
Haemostatic therapy with In a phase 2 trial in patients with ICH, rFVIIa (NovoSeven; Novo Nordisk Health Care, Bagsvaerd, Denmark) led to a reduction in HE (p=0·01) and Level 3A
rFVIIa improvement in neurological outcomes and mortality,8 but the phase 3 study (FAST trial), despite showing a statistically significant (p=0·009)
reduction in haematoma growth in rFVIIa-treated patients, did not show any functional or survival benefit;43 however, post-hoc analysis of the
FAST data suggests a potential benefit of rFVIIa in younger patients (<70 years) without known factors for poor outcome such as large haematoma
volume (<60 mL) or substantial IVH, if given within 2·5 h of the onset of symptoms44
AHA/ASA guidelines do not recommend rFVIIa for routine use in restricting HE in patients with ICH45
Blood pressure control In the INTERACT trial, the mean HE was 22·6% less at 24 h in the group that received intensive blood pressure control than it was in the Level 1B
guideline-based blood pressure control group (36·3%; p=0·04), but no statistically significant difference was recorded in functional outcome at
3 months between the two groups (median mRS score was 2 in both groups; p=0·66);20 a further subanalysis showed a beneficial effect of early
blood pressure reduction on HE, extending over 72 h46
In the ATACH phase 1 trial, in which patients were divided into tiers on the basis of blood pressure control (tier 1 being the highest level), HE was Level 1B
seen in 33% of patients in tier 1, 15% of patients in tier 2, and 22% of patients in tier 347
Surgery
Craniotomy A meta-analysis of ten trials of surgery for supratentorial ICH showed a benefit of surgery in primary supratentorial ICH on reduction of odds of an Level 1A
unfavourable outcome at follow-up; however, the authors noted that more trials were needed to make a definitive conclusion48
The STICH trial, which randomised 1033 ICH patients, showed no overall benefit of early surgery compared with initial conservative treatment for Level 1B
patients (26% vs 24% favourable outcome; p=0·41); however, a subgroup analysis showed that patients with haematoma within 1 cm of the
cortical surface benefited from early surgery, although this did not reach statistical significance (p=0·007)49
The AHA/ASA guidelines state the following:
(1) that evacuation of supratentorial ICH with standard craniotomy might be considered for patients presenting with lobar clots >30 mL and within Level 2b B
1 cm of the surface;45 and
(2) that surgical evacuation of infratentorial ICH is recommended as soon as possible for patients with cerebellar haemorrhage who are Level 1B
deteriorating neurologically or who have brainstem compression and/or hydrocephalus from ventricular obstruction2,45
Decompressive Evidence for the beneficial effect of decompressive surgery comes from small case series: in one series of 12 consecutive patients with a Level 2b B
craniectomy hypertensive ICH volume of >60 mL treated with decompressive craniectomy, 11 patients survived at discharge, of whom six had a good functional
outcome (mRS 0–3)50
In another case series of 23 patients with putaminal haematoma who underwent decompressive craniectomy, 13 patients had a good outcome and Level 2b B
10 had a poor outcome (including three deaths) at 90 days,51 suggesting that decompressive craniectomy might also have a role in the
management of patients
Minimally invasive surgery with stereotactic aspiration and thrombolysis
Alteplase The combination of frameless stereotactic aspiration and thrombolysis (FAST) in a phase 2 study of 28 patients with deep subcortical ICH showed Level 3B
the procedure to be safe and associated with reduction in ICH volume and early improvement on the NIHSS, with the potential to improve
outcome52
In another study of 15 patients who underwent frameless stereotactic aspiration and thrombolysis (FAST) of the clot, demonstrable ICH reduction ··
without perihaematoma enlargement was detected53
Urokinase Evidence for the potential beneficial effect of stereotactic infusion of urokinase on survival but not necessarily rebleeding has been provided by Level 2b B
randomised trials54–58
In a randomised controlled trial that compared 64 patients treated with MISPTT and 58 treated with conventional craniotomy, the MISPTT group Level 1B
had fewer complications and a trend towards improved short-term and long-term outcomes58
Image-guided Small randomised59,60 and non-randomised studies61–63 have shown the image-guided stereotactic endoscopic aspiration procedure to be effective Level 2b B
stereotactic endoscopic for immediate haematoma evacuation, with improved functional outcome and reduced mortality compared with best medical management61–63
aspiration In view of the uncertainty of the effectiveness of MIS for haematoma evacuation and the need for further research, the application of MIS with Level 2b B
either stereotactic or endoscopic aspiration with or without thrombolysis is not recommended for routine use2,45
AHA/ASA=American Heart Association/American Stroke Association. ATACH=Antihypertensive Treatment of Acute Cerebral Hemorrhage. FAST trial=Factor Seven for Acute Haemorrhagic Stroke trial.
HE=haematoma expansion. ICH=intracerebral haemorrhage. INTERACT=Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial. IVH=intraventricular extension of haemorrhage. MIS=minimally
invasive surgery. MISPTT=minimally invasive stereotactic puncture and thrombolysis therapy for acute intracerebral haemorrhage. mRS=modified Rankin score. NIHSS=National Institutes of Health Stroke Scale.
rFVIIa=recombinant factor VIIa. STICH=Surgical Trial in Intracerebral Haemorrhage. *The level of evidence is according to the Oxford Centre for Evidence-based Medicine (Level 1A being the highest level of evidence).64
Table 1: Management to restrict haematoma expansion
and Treating ICH Growth Study; NCT00810888) trials Both INTERACT 2 (NCT00716079) and ATACH 2
that are underway use the CT angiography spot sign (NCT01176565) are phase 2 trials underway to further
to stratify patients most at risk of HE who might benefit investigate the benefit of early BP reduction on HE and
from therapy with rFVIIa. However, rFVIIa is not clinical outcome in patients with ICH.
recommended at present for routine use to The role of surgical treatment for ICH is controversial.
restrict HE.45 Surgical procedures with varying amounts of supportive
Evidence from the INTERACT (Intensive Blood evidence include conventional craniotomy,48,49 minimally
Pressure Reduction in Acute Cerebral Haemorrhage invasive surgery (MIS),52–63,66 and decompressive crani-
Trial) and ATACH (Antihypertensive Treatment of Acute ectomy.50,51 Results from the STICH (Surgical Trial in
Cerebral Hemorrhage) trials show that SBP reduction Intracerebral Haemorrhage) trial49 showed no overall
might restrict HE in the hyperacute phase of ICH.20,46,47 benefit of early surgical clot evacuation compared with
www.thelancet.com/neurology Vol 11 January 2012 103
Review
Description Level of
evidence*
Reversal of The AHA/ASA recommend immediate reversal of anticoagulation;2,45 recommendations for reversal of anticoagulation in patients with ICH are as ··
anticoagulation follows:
Patients with a severe coagulation factor deficiency or severe thrombocytopenia should receive appropriate factor replacement therapy or platelets, Level 1C
respectively45
Patients with ICH whose INR is increased because of oral anticoagulants should have their warfarin treatment discontinued and receive therapy to Level 1C
replace vitamin K-dependent factors and to correct their INR45
Vitamin K (5–10 mg intravenously) remains an adjunct to initial therapy for OAC-associated haemorrhage because normalisation of INR can take up to Level 1C
24 h45
FFP (10–50 U/kg) is commonly used as an adjunct to vitamin K; it acts within a few h, but is associated with greater volume expansion, which might Level 2b B
precipitate heart failure, and requires much longer infusion times2
Prothrombin complex concentrates (10–50 U/kg), which act within a few min and have not shown improved outcome compared with FFP, might lead Level 2a B
to fewer complications than FFP and can be considered as an alternative to FFP45
rFVIIa (40–80 μg/kg), which acts within a few min, does not replace all clotting factors, and although the INR might be lowered, clotting might not be Level 3C
restored in vivo; rFVIIa is therefore not routinely recommended as a sole agent for OAC reversal in ICH45
The usefulness of platelet transfusions in ICH patients with a history of antiplatelet use is unclear and is considered investigational45 Level 2b B
Resumption of The decision as to whether to resume anticoagulation depends on analysis of the risk of recurrent haemorrhage balanced against the risk of ··
anticoagulation therapy thromboembolism because either complication can be associated with poor outcome and high mortality
after ICH The decision as to whether to resume anticoagulation should be based on underlying risk factors for recurrence: lobar location of the initial ICH, older Level 2a B
age (>65 years), ongoing anticoagulation, presence of the apolipoprotein ε2 or ε4 alleles, and greater number of microbleeds on MRI45
For nonvalvular AF, long-term anticoagulation should be avoided after spontaneous lobar ICH because of the high risk of recurrence, but antiplatelet Level 2a B
agents might be considered; antiplatelet treatment is probably safer than anticoagulation because it carries a substantially lower risk of bleeding2,40
Anticoagulation after non-lobar ICH might be considered depending on the indication2 Level 2a B
When to resume The optimum timing of the resumption of anticoagulation is a crucial issue with conflicting evidence:
anticoagulation A large retrospective study of 2869 patients with AF, mechanical heart valves, and additional risk factors for stroke with warfarin-related ICH suggests Level 2B
resumption of warfarin after about 10–30 weeks67
By contrast with reference 67, another systematic review of 492 patients concluded that anticoagulation might be resumed after 72 h68 Level 2A
A systematic review of six retrospective studies of 120 patients with mechanical heart valves and ICH concluded that resumption of warfarin within Level 2A
2 weeks is safe69
However, the AHA/ASA suggest that in patients with a very high risk of thromboembolism for whom restarting warfarin is considered, warfarin can be Level 2b B
restarted 7–10 days after ICH onset;2 the European Stroke Initiative recommends that warfarin can be restarted after 10–14 days70
Alternatives to warfarin Factor Xa and direct thrombin inhibitors are alternatives to warfarin, both of which might reduce the risk of thromboembolism with fewer bleeding ··
complications71
The direct thrombin inhibitor dabigatran (Pradaxa) has been shown to prevent ischaemic stroke to a similar extent as does warfarin, with reduced Level 1C
bleeding complications72
AF=atrial fibrillation. AHA/ASA=American Heart Association/American Stroke Association. ATACH=Antihypertensive Treatment of Acute Cerebral Hemorrhage. FFP=fresh frozen plasma. ICH=intracerebral
haemorrhage. INCH=International Normalized Ratio (INR) Normalization in Coumadin Associated Intracerebral Haemorrhage. OAC=oral anticoagulant. rFVIIa=recombinant factor VIIa. *The level of evidence is
according to the Oxford Centre for Evidence-based Medicine (Level 1A being the highest level of evidence).64
Table 2: Management of anticoagulant-associated intracerebral haemorrhage
initial conservative treatment in patients with ICH. Although decompressive hemicraniectomy is a life-
However, a subgroup analysis showed a potential benefit saving procedure for malignant middle cerebral artery
for surgery in lobar ICH within 1 cm of the cortical infarction, no randomised controlled trial has been done
surface.49 Pending the results of the STICH phase 2 trial in patients with ICH. The evidence for the potential
(NCT00716079), craniotomy is currently recommended beneficial effect of decompressive craniectomy comes
in selected patients with lobar clots of more than 30 mL from small case series.50,51 In the absence of further data,
and within 1 cm of the surface.2,45 both MIS and decompressive craniectomy are not
MIS is a promising option with many advantages over recommended for routine use in patients with ICH.2,45
conventional craniotomy, such as shorter surgery time, In anticoagulant-associated ICH (AAICH) the goal of
reduced tissue damage, and the fact that the procedure treatment is to rapidly normalise the international
can be done with local anaesthesia. The several methods normalised ratio (INR) and correct clotting factors
of MIS include stereotactic guidance with aspiration immediately (table 2). AAICH should be reversed
and thrombolysis with alteplase52,53,66 or urokinase,54–58 immediately with vitamin K and fresh frozen plasma or
and image-guided stereotactic endoscopic aspiration.59–63 prothrombin complex concentrate.45 The INCH (INR
The preliminary analysis of MISTIE (Minimally Normalization in Coumadin Associated Intracerebral
Invasive Surgery Plus rtPA for Intracerebral Haemorrhage; NCT00928915) trial comparing the use
Hemorrhage Evacuation; NCT00224770), an ongoing of fresh frozen plasma with prothrombin complex
evacuation trial combining stereotactic clot aspiration concentrate in patients with AAICH is underway.
with different doses of alteplase, suggests that MIS plus Further studies are needed to confirm the efficacy of
alteplase shows greater clot resolution than does con- platelet replacement or other interventions aimed at
ventional medical management.66 preventing or treating antiplatelet-related ICH because
104 www.thelancet.com/neurology Vol 11 January 2012
Review
Description Level of
evidence*
General Little evidence exists for the management of ICP in patients with ICH; data on the management principles for increased ICP in ··
considerations patients with ICH are based on guidelines for traumatic brain injury, which recommend maintenance of CPP at 50–70 mm Hg93
Reduction of increased ICP and maintenance at <20 mm Hg as well as maintenance of CPP at 50–70 mm Hg have become ··
therapeutic targets to prevent potentially life-threatening cerebral hypoperfusion45,93
Medical
Simple Simple non-interventional therapeutic manoeuvres for reduction of raised ICP include elevating the patient’s head to 30° and use Level 2a B
measures of analgesia and sedation2,45
Suggested drugs for analgesia and antitussive effect are morphine or alfentanil; propofol, etomidate, or midazolam are the ··
suggested drugs for sedation
Advanced More aggressive therapies for reducing ICP include osmotic diuretics (mannitol and hypertonic saline solution), drainage of CSF Level 2a B
measures through a ventricular catheter, neuromuscular blockade hyperventilation (with agents such as vecuronium or pancuronium),
and hypothermia2,45
Despite the beneficial effect of corticosteroids on vasogenic oedema (stabilisation of the capillary endothelial junction and Level 3B
reduction of cerebrovascular permeability), corticosteroids are contraindicated because randomised controlled trials showed
no efficacy in the treatment of oedema after ICH for lowering ICP and improving neurological deficit2
Concomitant monitoring of ICP and blood pressure to maintain CPP at >70 mm Hg is recommended when aggressive Level 2a B
measures are being used2
AHA/ASA guidelines recommend the consideration of ICP monitoring and treatment for patients with a Glasgow Coma Scale Level 2b C
score of 8 or less, those with clinical evidence of transtentorial herniation, or those with substantial IVH or hydrocephalus to
maintain CPP at 50–70 mm Hg, depending on the status of cerebral autoregulation45
Hypothermia A small pilot study of 12 patients with large ICH with mild endovascular hypothermia (35°C) for 10 days showed the following: Level 3C
hypothermia is safe and feasible in this patient group; hypothermia prevented the increase of PHE as compared with the matched
historical controls, in whom PHE volume doubled within 2 weeks; no rebound effect was recorded after rewarming, and all patients
survived during the 90 day follow-up period, unlike the historical control group, in which about 25% died because of an increase in
oedema and herniation within the first week of treatment;94 complications such as pneumonia, shivering, and bradycardia did not
seriously affect clinical course during the study
Neurosurgery Definitive neurosurgical interventions include craniotomy or ventriculostomy2 Level 2a B
AHA/ASA=American Heart Association/American Stroke Association. CPP=cerebral perfusion pressure. ICH=intracerebral haemorrhage. ICP=intracranial pressure.
IVH=intraventricular extension of haemorrhage. PHE=perihaematomal oedema. *The level of evidence is according to the Oxford Centre for Evidence-based Medicine
(Level 1A being the highest level of evidence).64
Table 3: Management of perihaematomal oedema and increased intracranial pressure after intracerebral haemorrhage
the usefulness of platelet transfusion in this group of stages of PHE formation after ICH. Whereas early PHE
patients is unclear.45 The decision as to whether or when is caused by the vasogenic effect of pro-osmotic
to restart anticoagulation therapy after ICH will depend substances (protein, electrolytes) from the clot, starting
on the risk of subsequent arterial or venous thrombo- immediately after bleeding and peaking at 4–5 days,76
embolism, the risk of recurrent ICH, and the clinical delayed PHE arises from a combination of vasogenic
state of the patient. and cytotoxic effects and lasts for 2–4 weeks.77 Within
Although guidelines from the American Heart the hyperacute first phase (a few hours post ictus) the
Association and American Stroke Association (AHA/ development of hydrostatic pressure during haematoma
ASA)2 suggest restarting warfarin 7–10 days after ICH formation and clot retraction leads to leakage of serum
onset in patients with a very high risk of thrombo- proteins from the clot into the surrounding tissue,
embolism, the European Stroke Initiative (EUSI) recom- resulting in vasogenic oedema.78 A second phase (which
mends starting warfarin after 10–14 days.70 begins a few days post ictus) results from activation of
the coagulation cascade and thrombin production.79 The
Perihaematomal oedema third, delayed phase (which begins days to weeks post
Clinical features ictus) is related to erythrocyte lysis and haemoglobin-
PHE, which is present in most patients with ICH, can mediated toxic effects caused by the iron-catalysed
be associated with increased mass effect and END14,73 production of reactive oxygen species.80,81
and is a predictor of poor functional outcome and Thrombin-induced activation of the inflammatory
mortality.1,73–75 PHE develops early in the hyperacute cascade and overexpression of MMPs is another
phase (increasing in volume by 75% in the first 24 h),75 potential mechanism that leads to blood–brain barrier
evolves over many days, and increases strongly during breakdown and PHE formation after ICH.79,82 MMPs
the first week 74 before it reaches its maximum during probably act by enhancing extracellular matrix
the second week after bleeding.1,14,76 proteolysis, damaging the basal lamina, and degrading
Although the mechanisms of oedema formation after c-Fn, a glycoprotein that is essential for haemostasis.83
ICH are not fully understood, several potential Radiological evidence of PHE formation after ICH
mechanisms have been postulated for the different has been provided by various studies.73–75,84–86 In the
www.thelancet.com/neurology Vol 11 January 2012 105
Review
A B C Management
The goal of therapy for PHE that occurs as a complication
of ICH is to prevent secondary brain insults, reduce ICP,
maintain blood supply and oxygen delivery, and optimise
cerebral metabolism. The treatment options for PHE and
increased ICP complicating ICH are mostly supportive
(table 3). Elevation of the head to 20–30° and avoidance of
pain and fever could minimise any rise in ICP. Medical
measures such as hyperventilation and the use of
analgesia, sedatives, and osmotic diuretics are designed
to lower ICP before placement of an ICP monitor or any
Figure 2: CT scans showing intraventricular extension of haemorrhage
A non-contrast CT showing left thalamic haematoma with extension of haemorrhage into the third ventricle
definitive neurosurgical intervention such as craniotomy
(A), a conventional contrast-enhanced CT showing two foci of active contrast extravasations (B), and follow-up or ventriculostomy.2 Placement of an ICP monitor is
non-contrast CT 12 h later showing pronounced haematoma growth with haemorrhage in both lateral recommended, especially in patients with a Glasgow
ventricles and severe hydrocephalus (C). Reproduced from Kim and colleagues,30 by permission of the American Coma Scale (GCS) score of less than 8 and those with
Journal of Neuroradiology.
transtentorial herniation.45
INTERACT study of patients with CT-confirmed ICH
who were assessed within 6 h of onset, PHE volume Intraventricular extension of haemorrhage and
increased within 72 h of the initial CT.84 In an MRI hydrocephalus
study, PHE volume increased most rapidly in the first Clinical features of IVH
2 days after symptom onset and peaked towards the end IVH is common after ICH, occurring in 30–50% of
of the second week.86 patients, and is a major additional predictor of poor
Other factors that have been proposed to affect PHE prognosis (figure 2).9–11,95–97 A relation exists between the
volume include hyperglycaemia, coagulation factors, location and volume of ICH and the presence of IVH.11,95
and use of statins.86,87 Likewise, increased serum A subanalysis of the activated rFVIIa phase 2 trial showed
concentrations of MMP-988,89 and persistently increased a relation between thalamic ICH and increased frequency
SBP90 are associated with an increased PHE volume. of IVH.11 This was attributable to the anatomical closeness
Although the possible presence of an ischaemic of the thalamus to the third ventricle and the
penumbra around the area of the ICH—leading to predisposition for blood to spread medially.11,95
secondary neuronal injury and cytotoxic oedema—was Hallevi and colleagues95 calculated a decompression
previously a concern, evidence against a peri- range for each location of ICH, the range of ICH volume
haemorrhagic penumbra has since been provided by within which IVH is more likely to occur during the
MRI and perfusion CT studies, which have linked acute phase of ICH as the haematoma enlarges and
perihaematoma hypoperfusion to reduced metabolic below which ICH is unlikely to be complicated by IVH.
demand rather than tissue ischaemia.91,92 They noted a narrow decompression range for thalamic
The oedema volume can exceed that of the original and pontine haemorrhages, a wide range for lobar ICH,
haematoma, leading to substantial additional mass and a non-measurable decompression range for caudate
effect with tissue shifts, and might contribute to further haemorrhage.95
neuronal injury and poor outcome after ICH.14,73,74,80 Several studies have shown that IVH in patients with
Also, rapidly developing PHE could lead to increased ICH is an independent predictor of poor functional
ICP or obstructive hydrocephalus and subsequent outcome and higher mortality,9–11,43,49,75,95,98 with a reported
herniation.80 The increased ICP resulting from overall mortality rate of 50–75%.75,99–101 The 30 day mortality
surrounding PHE can contribute to brain injury and rate was shown to be 43% in ICH patients with IVH
END, and to reduced cerebral perfusion pressure.45 compared with 9% in those without.9 In the rFVIIa trial,
Evidence for an effect of PHE on clinical outcome and although 38% of 375 patients with ICH had IVH at
mortality after ICH is unclear: although some obser- baseline, 45% had developed IVH by 24 h after presentation.
vational studies have recorded an association between A good functional outcome (mRS 0–3) was achieved by
PHE and poor outcome,73,74,80 another study detected no 43% of the patients without IVH at presentation compared
clear association.75 Also, in another study, absolute with only 20% of those with IVH at baseline. Similarly, out
oedema volume growth was correlated with a decrease of the group that had IVH growth in the first 24 h, only 7%
in neurological status at 48 h after ICH, but not with had a good functional outcome (mRS 0–3) at 90 days.11 A
3 month functional outcome.86 mean arterial pressure (MAP) of greater than 120 mm Hg
In the INTERACT trial, both absolute and relative at baseline, a large baseline ICH volume, and the presence
growth in PHE volume were associated with mortality of IVH at presentation were identified as risk factors for
or dependency at 90 days after adjustment for age, sex, IVH growth.11 Both the presence of IVH at any time and
and randomised treatment, but not when further IVH growth increased the likelihood of death or severe
adjusted for baseline haematoma volume.84 disability at 90 days.11
106 www.thelancet.com/neurology Vol 11 January 2012
Review
In the subanalysis of the STICH trial, only 15% of the Management
377 patients with IVH had good (normal, good, or The aim of treatment in ICH patients with IVH and
moderate recovery) Glasgow Outcome Scale functional hydrocephalus is to evacuate the intraventricular
outcomes, compared with 31% of the 375 ICH patients haematoma, thus relieving the obstruction to CSF flow,
without IVH.10 reversing ventricular dilatation, and restoring normal
Proposed mechanisms for the deleterious effects of intracerebral pressure (table 4). Insertion of external
IVH on mortality and morbidity include damage to ventricular drainage (EVD) can be a life-saving procedure,
periventricular brain structures, especially the brainstem, relieving acute hydrocephalus and subsequent herniation
complications of acute obstructive hydrocephalus, and in ICH patients with severe IVH and AOH.97,100,108 EVD is
IVH-induced inflammatory response, possibly due to recommended for the treatment of hydrocephalus in
blood and its breakdown products.10,102,103 patients with decreased consciousness.45
The volume of IVH affects morbidity and mortality at Because EVD is often occluded by blood clots, leading
30 days.11,98,104 A review of 47 patients with ICH by Young to inadequate CSF drainage, thrombolytics can be
and colleagues98 identified a lethal volume of 20 mL, instilled into the ventricles to maintain EVD functionality
above which patients had a poor outcome. Similarly, and promote fast clearance of the ventricles.106,109–117
early expansion of IVH worsens clinical outcome and Findings from the CLEAR IVH (Clot Lysis: Evaluating
increases mortality to 50–75%.9 Accelerated Resolution of Intraventricular Hemorrhage)
Although IVH volume in itself is associated with poor phase 2 trial117 suggest that low-dose alteplase can be safe
outcome, an even stronger association exists between the and might increase the lysis rate. However, pending the
total (ICH plus IVH) volume and adverse outcomes.1,10,95,98,104 results of the ongoing CLEAR phase 3 trial (NCT00784134),
Another study identified a 40 mL total volume as a cutoff routine clinical use of intraventricular fibrinolysis is not
value, above which patients were 41 times more likely to recommended.45 Other treatment options include
have a poor prognosis, and 50 mL as a poor outcome endoscopic surgical evacuation of the haemorrhage118–120
threshold, above which 100% of patients would have an and the less-invasive lumbar drainage.97,107,122
unfavourable outcome.104
Seizures and epilepsy
Clinical features of hydrocephalus Clinical features
Extension of haemorrhage into the ventricles can impede Seizures are a frequent complication of ICH and can
normal CSF flow and, with direct mass effects of even be the presenting symptom.123 Seizures most
ventricular blood, lead to acute obstructive hydrocephalus commonly occur at the onset of ICH, but can be delayed.
(AOH). AOH can be a life-threatening disorder, especially About 50–70% of seizures occur within the first 24 h, and
if the third and fourth ventricles are affected.9–11 Up to 90% in the first 3 days,124–127 with an overall 30 day risk of
50% of patients with IVH secondary to ICH can develop seizures of about 8%.123
hydrocephalus caused by obstruction of the third and Early seizures are defined as those occurring within
fourth ventricles by ventricular clots.105 2 weeks of initial ictus, late seizures occurring there-
Many studies have shown involvement of the third and after.124,125 Whereas early seizures are thought to be caused
fourth ventricles in patients with IVH after ICH to be by structural disruption and cellular biochemical
predictive of adverse outcome and high mortality.9–11,105 In dysfunction, late seizures are attributed to gliosis and the
a subanalysis of CT images from the STICH trial, the development of meningocerebral cicatrices.124,125 Early
presence of hydrocephalus reduced the likelihood of seizures can be predictive of epilepsy development.128
positive outcome from 15·1% to 11·5%.10 The incidence of seizures after ICH varies widely
Acute hydrocephalus is more common in patients with depending on study design, diagnostic criteria, duration
high IVH volume (Graeb score ≥6) than it is in patients of follow-up, and the population studied. Similarly, the
with low to moderate IVH volume (Graeb score ≤6).101 true incidence of seizures might be underestimated,
Hydrocephalus occurs more with thalamic than with because subclinical seizures can be detected with use of
putaminal haemorrhages and is almost absent in the continuous EEG (cEEG) monitoring only. Overall
case of lobar haemorrhages, probably because small incidence after ICH is 4·2–20%123,124,127,129,130 for clinical
thalamic haemorrhages can easily compress the cerebral seizures and 29–31% for subclinical seizures.125,126,131 In a
aqueduct leading to obstruction to normal CSF flow and series of 63 patients with ICH in an intensive care unit
subsequent hydrocephalus, whereas small ganglionic (ICU) who had cEEG monitoring within 72 h of
haemorrhages rarely have any effect on ventricular admission, non-convulsive seizures were detected in
size.98,105 Communicating hydrocephalus can develop with 28%, four times the incidence of observable seizures.
impairment of the Pacchioni granulations by ventricular The presence of seizures was independently associated
haemorrhage.97,106,107 Increased ICP can result from large with increased midline brain shift on 48–72 h follow-up
volume ICH, especially in the presence of IVH with head CT scans, with neurological deterioration.126
hydrocephalus, leading to further clinical deterioration In a retrospective review125 of 102 patients with ICH
and poor outcome.9–11 with cEEG monitoring, 19% had convulsive seizures,
www.thelancet.com/neurology Vol 11 January 2012 107
Review
Description Level of evidence*
External EVD insertion has been suggested as a life-saving procedure in patients with ICH with severe IVH and AOH through reduction of ICP and subsequent Level 2b C
ventricular herniation;97,100,108 however, the complications of EVD include occlusion by blood clots leading to inadequate CSF drainage,97,100 infections leading to frequent
drainage EVD exchange,96,107,109 and CH caused by impairment of the Pacchioni granulations by IVH107
AHA/ASA guidelines recommend that:
Patients with a GCS score of 8, those with clinical evidence of transtentorial herniation, or those with substantial IVH or hydrocephalus should be considered Level 2b C
for ICP monitoring and treatment; treatment should aim to maintain a CPP of 50–70 mm Hg, depending on the status of cerebral autoregulation45
Ventricular drainage as treatment for hydrocephalus should be considered in patients with a decreased level of consciousness45 Level 2a B
Intraventricular Compared with ventriculostomy alone, IVF with either urokinase106,109 or alteplase110–112 has been shown to promote early and effective clearance of blood in Level 2b B
fibrinolysis the ventricles, maintain EVD functionality, and reduce the need for permanent shunts as well as improve clinical outcome and reduce mortality;
the benefits of IVF might be offset by complications such as secondary haemorrhage and EVD infection111,113,114
IVF can reduce the mortality rate from a range of 60–90% to only 5%;112 two systematic reviews of clinical studies recorded a 30–50% reduction in mortality Level 2a B
after IVF115,116
Improved short-term outcome in patients with EVD and IVF can improve 30 day106 and 90 day outcome,111 but not long-term outcome after 12 months110 Level 2B
In the CLEAR IVH phase 2 trial, designed to assess the safety of open-label doses of intraventricular alteplase in 52 patients with IVH, one dose of 1 mg Level 3B
alteplase and a dosing interval of 8 h was shown to be the most appropriate dosing for IVH,117 suggesting that low-dose alteplase can be safely given to treat
stable intraventricular clots and can increase the lysis rates; symptomatic bleeding occurred in 4% and bacterial ventriculitis in 2% of patients with a 30 day
mortality rate of 17%117
AHA/ASA guidelines do not recommended the routine use of IVF in clinical practice45 Level 2bB
Endoscopic Evidence for the potential beneficial effect of neuroendoscopic surgical removal of IVH comes from observational studies:118–121 in one study, 24 of 25 patients Level 3B
surgical who had ESE of IVH and obstructive hydrocephalus had resolution of hydrocephalus;120 similarly, in another study of 17 patients with IVH and hydrocephalus
evacuation treated with ESE, all patients had successful resolution of hydrocephalus with good outcomes;121 and in a non-randomised comparison study, patients treated
with ESE of IVH had a higher rate of good recovery at 2 months than did those treated with EVD119
Lumbar LD is an alternative option for extracorporeal CSF drainage in patients with CH and has been shown to be a simple, safe, and less invasive procedure; it avoids ··
drainage the need for EVD exchange and can substantially reduce the incidence of permanent hydrocephalus and the need for shunt surgery; it also has a lower
complication profile than does EVD97,107,122
In a prospective case series of three patients, the combination of IVF and LD was shown to be a simple and promising alternative for the treatment of CH after Level 1C
ICH and IVH122
In a retrospective analysis of 16 patients with persisting CH after secondary IVH who received an EVD and concurrent LD compared with 39 historical patients Level 2b C
treated with EVD alone, LD replaced the need for repeated EVD exchanges, extending the duration of extracorporeal CSF drainage (16 days EVD vs 21 days
EVD plus LD) and eventually reducing the need for a permanent ventriculoperitoneal shunt (18·75% vs 33%; p<0·03) in LD-treated patients107
In a prospective study, 32 patients with ICH and severe IVH with AOH received an EVD (n=32), and of the 28 patients who developed CH, early LD replaced the Level 1C
need for EVD, with one patient requiring a shunt; the additional treatment with either IVF or LD reduced the incidence of EVD exchange (to 32% and 40%,
respectively) and shunt surgery (to 18%)97
AHA/ASA=American Heart Association/American Stroke Association. AOH=acute obstructive hydrocephalus. CH=communicating hydrocephalus. CLEAR IVH=Clot Lysis: Evaluating Accelerated Resolution of
Intraventricular Hemorrhage. CPP=cerebral perfusion pressure. ESE=endoscopic surgical evacuation. EVD=external ventricular drainage. GCS=Glasgow Coma Scale. ICH=intracerebral haemorrhage.
ICP=intracranial pressure. IVF=intraventricular fibrinolysis. IVH=intraventricular extension of haemorrhage. LD=lumbar drainage. *The level of evidence is according to the Oxford Centre for Evidence-based
Medicine (Level 1A being the highest level of evidence).64
Table 4: Management of ventricular extension of haemorrhage and hydrocephalus
13% had electrographic seizures, and 5% had both, with account for seizures early in ICH.124 Early-onset seizures
94% of the seizures detected in the first 72 h. Subclinical are thought to be directly related to the insult of ICH to
seizures were associated with expanding haemorrhages, the brain.127
especially if they expanded by more than 30% in the Identified predisposing factors include haemorrhagic
first 24 h or if they reached the cortex, and were also size, the presence of hydrocephalus, intracranial midline
associated with a poor outcome. Electrographic seizures shift, low GCS, and severe neurological deficit.124 Lobar
were twice as common (31% vs 14%) in patients with location is an independent predictor of early seizures.123
expanding haemorrhages.125 Non-occipital lobar haemorrhages,125–127,133 as well as
The reported frequency of status epilepticus is subcortical haemorrhages,126 are commonly associated
0·3–21·4%.130,132,133 In an earlier study of 1402 patients with with seizures.
ICH, status epilepticus occurred in 11 of 65 patients with Conflicting results on the association of seizures after
seizures and was the initial presentation of ICH in six of ICH with clinical outcome and mortality have been
these 65 patients.130 Epilepsy (recurrent seizures) has reported. In one study,134 the in-hospital mortality rate
been reported to develop in 2·5–4% of patients,124,130 but was 37·9% in patients with both acute ICH and IS with
Passero and colleagues123 reported the risk of late seizures seizures within 48 h of symptom onset compared with
or epilepsy in survivors of ICH to be 5–27%. Recurrent 14·4% for patients without seizures. Another study128 of
seizures occurred in four of 14 patients in one study, ICH and IS showed an increased risk of mortality within
despite the provision of antiepileptic treatment.133 30 days if seizures developed within the first 24 h after
Although the cause of seizures in patients with ICH is stroke (32·1% vs 13·3%). Although mortality rates were
unclear, the combination of sudden development of a higher in patients with seizures, seizures were not an
space-occupying lesion with mass effect, focal ischaemia, independent predictor of mortality at 30 days or of poor
and blood breakdown products has been postulated to outcome post stroke after adjusting for other factors,
108 www.thelancet.com/neurology Vol 11 January 2012
Review
Description Level of evidence*
General No randomised controlled trials have been done to guide decisions on seizure prophylaxis or treatment in patients with ICH; however, AHA/ASA guidelines45 ··
considerations recommend the following:
Patients with clinical seizures should be treated with AEDs Level 1A
Patients with a change in mental status who have electrographic seizures on EEG should be treated with AEDs Level 1C
EEG monitoring is indicated in ICH patients with depressed mental status that is out of proportion with the extent of brain injury Level 2a B
Antiepileptic The choice of initial AED depends on individual circumstance and contraindications; the AEDs to be considered for the acute treatment of ··
drugs post-haemorrhagic stroke seizures include intravenous lorazepam (0·05–0·10 mg/kg) followed by a loading dose of phenytoin or fosphenytoin
(15–20 mg/kg), valproic acid (15–45 mg/kg), levetiracetam (500–1500 mg), or phenobarbital (15–20 mg/kg)
Prophylaxis The benefit of seizure prophylaxis after ICH is controversial: some investigators have advocated the use of prophylaxis in most patients126 and previous ··
guidelines2,70 have recommended a 30 day course of prophylactic AEDs in patients with lobar haemorrhage or those who have had seizures, on the basis
of risk reduction of seizures in patients with lobar haemorrhage reported in observational studies123
However, two observational studies have since shown prophylactic therapy with AEDs to be associated with poor outcome:136,137 in a prospective study of Level 3B
98 patients with ICH, prophylactic phenytoin was associated with higher fever and worse outcome at 14 days or at discharge, and worse functional
outcome at 14 day, 28 day, and 3 month follow-up;136 similarly, in another trial, an association was recorded between AED use and worse 3 month
functional outcome137
In the absence of data for patients with ICH showing a benefit of seizure prophylaxis, the most up-to-date AHA/ASA guidelines recommend against Level 3B
prophylactic use of AEDs45
AEDs=antiepileptic drugs. AHA/ASA=American Heart Association/American Stroke Association. ICH=intracerebral haemorrhage. *The level of evidence is according to the Oxford Centre for Evidence-based
Medicine (Level 1A being the highest level of evidence).64
Table 5: Clinical management of seizures and epilepsy after intracerebral haemorrhage
although the risk in patients with ICH was not Venous thromboembolic events
independently determined.128 Clinical features
Findings from one study126 showed that post-ICH VTE are a common and potentially fatal complication in
seizures are associated with worsening neurological patients with ICH that can manifest as either deep-vein
function as measured with the NIHSS (National thrombosis (DVT) or pulmonary embolism (PE).138,139 The
Institutes of Health Stroke Scale), and recorded a trend reported rate of clinically symptomatic VTE is 3–7%.138,140,141
towards increased poor outcome, with a mortality rate of Overall, studies have estimated the short-term post-ICH
27·8% compared with 15% in those without seizures.126 risk of PE to be 1–2% and of DVT to be 1–4%.138 Subclinical
However, other studies have recorded no substantial DVT is more common than is clinically apparent DVT,
difference in mortality between patients with or without with asymptomatic DVT rates occurring in up to 17% of
seizures after stroke,124 and, surprisingly, there was an patients with ICH.142 In a small prospective study of
association with better outcomes after stroke as measured 52 patients with acute ICH, DVT was detected in 40% of
with Scandinavian stroke scales.135 patients within 2 weeks, with one case of PE recorded.143
The high rate was attributed to the extent of paralysis due
Management to severe stroke. In the rFVIIa trial,8 about 2% of patients
No randomised controlled trials (RCTs) have been done in both the placebo and treatment groups developed
to guide decisions on seizure prophylaxis or treatment DVT, and about 2% developed PE.8
in patients with ICH. Similarly, no definitive evidence DVT is a risk factor for PE. PE generally arises from
or clear guidelines exist for the choice of treatment or venous thrombi that develop in a paralysed lower leg or
duration of treatment for patients with one or more pelvis.144 However, about 30% of patients diagnosed with
seizures or status epilepticus (table 5). However, acute PE show no evidence of DVT in their lower legs,
available guidelines recommend that patients with implying that a negative venous duplex ultrasound does
clinical seizures should be treated with antiepileptic not exclude the diagnosis of acute PE.145
drugs (AEDs).45 The choice of initial AED is dependent Independent risk factors associated with the
on the individual characteristics of each patient, development of VTE in patients with ICH include severe
including medical comorbidities, concurrent drugs, and stroke, lengthy immobilisation, advanced age, and
contraindications. The benefit of seizure prophylaxis increased prothrombotic activity.143,146 Discontinuation of
after ICH is controversial. Whereas previous studies antithrombotic agents after ICH could also accelerate the
have advocated the use of prophylaxis in most formation of DVT.143
patients,123,136 two observational studies have since shown Although a high D-dimer value is a useful predictor of
prophylactic therapy with AEDs to be associated with DVT formation in patients with ICH, this value could
poor outcome.136,137 Whereas previous guidelines2,64 have also be increased because of the presence of infection or
recommended a 30 day course of prophylactic AED in hyperfibrinolysis caused by the cessation of anti-
patients with lobar haemorrhage or those who have had coagulation.143
seizures, the most up-to-date guideline recommends In a retrospective study of symptomatic VTE in patients
against prophylactic use.45 with ICH, the most commonly identified risk factors were
www.thelancet.com/neurology Vol 11 January 2012 109
Review
age (>40 years), immobility due to paresis or restrictions hypothalamic stroke164—patients with IVH are thought to
for mechanical ventilation, presumed infection, and the have more of a neurogenic or central fever.166
presence of an indwelling central venous catheter.141 A high body temperature after ICH is associated with
A systematic review detected racial disparity in the HE, cerebral oedema, increased ICP, and END.45,169 Fever
incidence of VTE after ICH, with a higher rate of DVT in after ICH is associated with longer ICU and hospital
black patients than in white patients after adjusting for stays, poor functional outcome, and increased mortality.167
differences in the risk factors for ICH.147 A sex difference A prospective study of 390 mixed ischaemic and
also exists, with women being at greater risk of VTE.139,148 intracerebral haemorrhagic stroke patients (9% with
VTE is associated with a 30 day mortality rate ICH) admitted within 6 h of stroke onset showed that the
of 35–52%.2 In the Oxford Community Stroke Project, relative risk of poor outcome increased by 2·2 times and
5% of patients with ICH died of PE within the first that mortality increased by a factor of 1·8 for each 1°C
30 days.3 Both DVT and PE can slow down rehabilitation increase in baseline body temperature.166
and recovery, and extend the duration of hospital stay.144 In a subanalysis of data from the PAIS (Paracetamol
[Acetaminophen] In Stroke) trial168 of 1332 IS and ICH
Management patients admitted within 12 h of stroke onset, 10% of
A clinical dilemma can arise as to the best possible 163 ICH patients had admission body temperatures of
approach to VTE prevention in patients with ICH, because more than 37·5°C. An early rise in body temperature
anticoagulants can increase the risk of HE or rebleeding. rather than high body temperature on admission was the
Although this decision is often made on the basis of a risk– greatest risk factor for adverse outcome.164
benefit analysis in the context of the individual patient, In a study of 251 cases of ICH, initial body temperature
prophylaxis for VTE in patients with ICH has been was not an independent prognostic factor, but an increase
addressed in some guidelines.2,149 Options for reducing the in body temperature during the first 72 h, which occurred
risk of VTE after ICH include intermittent pneumatic in 91% of patients, was associated with poor clinical
compression, low-dose subcutaneous low-molecular- outcome. Also, for those patients surviving the first 72 h
weight heparin or unfractionated heparin (table 6).2,45 after hospital admission, a longer duration of fever was
An even greater clinical therapeutic dilemma is the associated with a worse outcome.163
management of patients with ICH who subsequently In a retrospective study of 330 patients with acute IS
develop VTE. If untreated, the risk of recurrent fatal PE is and ICH, of the 37·6% of 330 patients who had fever,
increased and, if treated, patients are at increased risk of 22·7% had a documented infection and 14·8% had fever
bleeding. Anticoagulation has been estimated to double without a documented infection.170 Reith and colleagues166
the risk of recurrent ICH compared with the overall detected infection in a fifth of the 25% of mixed IS and
recurrence risk of ICH, and the mortality rate associated ICH pyrexial patients (body temperature >37·5°C on
with recurrent ICH can be as high as 50%.160 The risk of admission within 6 h of stroke onset). Pulmonary and
recurrent ICH can depend on factors such as the patient’s urinary infections are the main causes of infectious fever
age and the location of ICH. Patients with lobar in patients with stroke.162,163,168,171 In the PAIS study, most
haemorrhages are at higher risk of rebleeding, probably infectious fevers were due to pneumonia and urinary
due to suspected amyloid angiopathy.161 tract infections (UTIs).168 In the review with only ICH
Insertion of a vena cava filter is recommended in patients, pulmonary infection was diagnosed within the
patients with ICH who develop an acute proximal venous first 72 h in 84 patients (43% of 196 patients) and UTI was
thrombosis. The decision to start antithrombotic diagnosed within the same time in 69 patients (35% of
treatment several weeks after the vena cava filter should 196 patients).163
be made on the basis of a risk–benefit analysis of the
potential for rebleeding as well as the patient’s co- Management
morbidities and mobility.2 ICH patients with a high temperature should be
physically examined and investigated to establish the
Fever cause of fever and possibly the source of infection.
Clinical features Generally, treatment with antipyretics and cooling
Fever occurs in up to 40% of patients after ICH,162,163 and is blankets is used169 for patients with a sustained fever of
independently associated with a poor outcome and more than 38·3°C (panel). Although new adhesive
increased mortality.163–167 The incidence of fever surface-cooling systems and endovascular heat-exchange
(temperature >38·3°C) is high in basal ganglionic and catheters might prove more effective,171,173 they have not
lobar ICH, especially in patients with IVH.45,162,163 The cause been systematically investigated in patients with ICH. No
of high temperature after stroke is not always apparent, evidence is available from RCTs linking fever treatment
although increased body temperature might be a direct with improved clinical outcome or reduced mortality. A
consequence of brain damage caused by stroke or Cochrane review showed no statistically significant effect
accompanying infections.164,168 Increased body temperature of pharmacological or physical temperature-lowering
could result from damage to the thermostatic centre after therapy in reducing the risk of death or dependency.172 In
110 www.thelancet.com/neurology Vol 11 January 2012
Review
Description Level of evidence*
Prevention
Non- On the basis of findings from a randomised controlled trial that showed intermittent pneumatic compression combined with elastic stockings to be Level 1B
pharmacological better than elastic stockings alone in the reduction of the rate of asymptomatic DVT after ICH (4·7% vs 15·9%)142 and the finding that graduated
approaches compression stockings alone are ineffective in preventing DVT,150 AHA/ASA guidelines recommend that patients with ICH should have intermittent Level 1B
pneumatic compression for prevention of venous thromboembolism in addition to elastic stockings2,45
Pharmacological Randomised trials,144,151 a non-randomised study,152 and a retrospective study140 have shown pharmacological prophylaxis with LMWH for DVT and PE Level 2b B
approaches prevention 24–48 h after ICH to be safe with no increased risk of haematoma expansion or further bleeding, although LMWH has not been shown to
be better than elastic stockings
On the basis of these studies, AHA/ASA guidelines suggest that after cessation of bleeding, low-dose subcutaneous LMWH or unfractionated heparin can Level 2b B
be considered for prevention of venous thromboembolism in patients who are immobile after 1–4 days from onset of ICH45
Treatment
IVC filters Insertion of an IVC filter is an option for patients who cannot receive therapeutic anticoagulation or for those who have to wait for several weeks ··
before starting anticoagulation;153–156 IVC filters prevent PE by trapping most of the large emboli originating from the deep veins of the pelvis and
feet,157 but the benefits can by counterbalanced by complications such as venous thromboembolism and caval occlusion, with no difference in
mortality153–156
A retrospective review of 371 mixed stroke patients (105 [28%] with ICH) who received an IVC filter recorded a 16% incidence of symptomatic Level 2b C
post-filter DVT, a 0·8% incidence of post-filter fatal PE, and a 5·1% incidence of caval occlusion; other filter-related complications included fracture of
filter, penetration of caval wall, and filter migration156
No randomised controlled trial has compared vena cava filters with anticoagulation in patients with ICH or ischaemic stroke; nonetheless, in the Level 1B
PREPIC randomised controlled trial of 400 patients with documented proximal DVT or PE who received concurrent anticoagulation, IVC filters
reduced the risk of PE, even after 8 years, although there was an associated long-term risk of recurrent DVT but no statistically significant reduction in
mortality, probably because of the older study population, and most deaths were due to cancer or cardiovascular diseases158
Similarly, an earlier randomised study comparing the effectiveness of a combination of anticoagulation and IVC filters versus anticoagulation alone in Level 1B
patients with proximal DVT showed a statistically significant decrease in the incidence of PE in the filter group (1·1% vs 4·8%); there was, however, a
subsequent excess of recurrent DVT, without any difference in mortality153
The AHA/ASA and international guidelines recommend that patients with ICH who develop an acute proximal DVT, particularly those with clinical or Level 2b C
subclinical PE, should be considered for acute placement of a vena cava filter2,149
Anticoagulation The AHA/ASA guidelines recommend that the decision to start antithrombotic therapy several weeks after the placement of a vena cava filter must be Level 2b B
made on the basis of a risk–benefit analysis of the potential for recurrent bleeding (amyloid-related ICH has higher risk of recurrent ICH than does
hypertension-related ICH), as well as associated disorders with increased arterial thrombotic risk (eg, atrial fibrillation), and the overall health and
mobility of the patient2
Surgical The evidence for the benefit of surgical embolectomy as a life-saving procedure for PE as a complication of ICH comes from case series: in one series of Level 3C
embolectomy three consecutive cases of pulmonary embolectomy in patients with ICH with massive PE, the interval between the onset of intracranial bleeding and
emergency surgical embolectomy was 7–16 days, and all three patients survived without any neurological exacerbation;159 however, the problem
associated with surgical embolectomy is the possible exacerbation of intracranial bleeding from systemic heparinisation
AHA/ASA=American Heart Association/American Stroke Association. DVT=deep-vein thrombosis. ICH=intracerebral haemorrhage. IVC=inferior vena cava. LMWH=low-molecular-weight heparin.
PE=pulmonary embolism. PREPIC=Prévention du Risque d’Embolie Pulmonaire par Interruption Cave. *The level of evidence is according to the Oxford Centre for Evidence-based Medicine (Level 1A being
the highest level of evidence).64
Table 6: Prevention and clinical management of venous thromboembolic events after intracerebral haemorrhage
the PAIS RCT,168 no difference was seen between the outcome,12,32,174–176 and that it is a potent predictor of 30 day
placebo group and the group treated with paracetamol in mortality in both diabetic and non-diabetic patients with
patients with IS and ICH within 12 h of symptom onset. ICH13 as well as an independent predictor of early
However a post-hoc analysis of patients with a baseline mortality and worse functional outcome in non-diabetic
body temperature of 37–39°C who were treated with patients with ICH.175,176
paracetamol showed improved outcome. Sources of In the post-hoc analysis of the ATACH trial of
infectious fever should be treated with appropriate 60 patients, the risk of poor outcome (mRS 4–6) in
antibiotics, and antipyretics should be given to lower patients with persistent or increasing serum glucose
temperature in ICH patients with fever.2 concentrations was more than twice that of patients with
a reduction in serum glucose concentrations (relative
Hyperglycaemia risk [RR]=2·64, 95% CI 1·03–6·75). Also, the RRs were
Clinical features 2·59 (1·27–5·30) for HE of more than 33%, and 1·25
A high proportion of patients (about 60%) might develop (0·73–2·13) for a relative oedema expansion of more
hyperglycaemia even in the absence of a previous history than 40%.177
of diabetes after ICH.174 Increased blood glucose in the
acute setting of ICH is probably a response to stress and Management
severity of ICH13 and can persist for up to 72 h after Poor outcomes associated with hyperglycaemia could be
ICH.174 avoided or minimised through monitoring glucose and
Many studies have shown that increased serum glucose maintaining normoglycaemia (table 7). Control of
on admission is associated with larger haematoma size, hyperglycaemia in the acute setting of ICH decreases the
HE, PHE, cell death, and increased risk of poor likelihood of HE, PHE, ICP, and seizures, and improve
www.thelancet.com/neurology Vol 11 January 2012 111
Review
multifactorial process that includes activation of the
Panel: Clinical management of fever and infection after intracerebral haemorrhage neuroendocrine systems (sympathetic nervous system,
The goal should be to maintain normothermia and treat infections in patients with glucocorticoid system, or the renin–angiotensin axis),
ICH. Patients with ICH and sustained fever in excess of 38·3°C should be treated with increased cardiac output, and stress response to
antipyretics and cooling blankets163,169 (Level 1C). However, there is no evidence from conditions such as increased ICP, headache, and
randomised controlled trials to link fever treatment with improved clinical outcome or urinary retention.45,180,182
reduced mortality. A Cochrane review of five pharmacological temperature-lowering Many studies have shown an association between
trials and three physical cooling trials with 423 participants recorded no statistically increased BP in the acute phase of ICH and HE, PHE,
significant effect of pharmacological or physical temperature-lowering therapy in and rebleeding.19,36,37,90 Increased BP in the acute setting of
reducing the risk of dependency (odds ratio 0·9, 95% CI 0·6–1·4) or death (0·9, ICH is associated with worse outcome and increased
0·5–1·5)172 (Level 1C). Equally, an updated meta-analysis of a Cochrane review with six mortality.180,182,183 In a large study of 3930 mixed stroke
pharmacological temperature-lowering therapies did not show any statistically patients (1760 with ICH), the in-hospital case-fatality rate
significant difference between the treated and placebo groups in the proportion of was 5·9% for patients with ICH. Also, both SBP and
patients who were alive and independent (modified Rankin score ≤2) at final follow-up diastolic BP were associated with odds of death or
(1·1, 0·9–1·3)168 (Level 1C). In PAIS, a randomised controlled trial, treatment with disability in such patients.183
high-dose acetaminophen (6 g daily) in 1400 patients with ischaemic stroke and ICH However, the effect of BP levels on mortality seems to
within 12 h of symptom onset was associated with a 0·26°C (95% CI 0·18–0·31) conform to a U-shaped distribution after ICH, as poorer
reduction in mean body temperature measured 24 h after admission; the trial did not outcomes have also been seen at very low SBP
provide sufficient evidence to lend support to routine use of high-dose paracetamol in (<120 mm Hg) and at very high (>220 mm Hg) SBP
patients with acute stroke. However, in a post-hoc analysis of patients with a baseline values.184
body temperature of 37–39°C treated with paracetamol, a 9% absolute increase was
recorded in the number of patients with improved outcome, with a number needed to Management
treat of 11; serious adverse events occurred in 8% of the paracetamol group versus 10% The poor outcome associated with increased BP after
of the placebo group (Level 1B). Although no evidence from randomised controlled ICH could be minimised with BP monitoring and
trials is available to lend support to the routine use of physical or pharmacological treatment aimed at maximisation of cerebral perfusion
strategies to reduce temperature in patients with acute stroke, the AHA/ASA guidelines while minimising ongoing bleeding (table 8). The
recommend that the sources of fever should be treated with appropriate antibiotics rationale for lowering BP after ICH is because SBP
and that antipyretic drugs should be given to lower temperature in febrile patients reduction can reduce the rate of HE and possibly improve
with ICH (Level 1C).2 clinical outcome.
The INTERACT trial showed that a reduction of SBP to
AHA/ASA=American Heart Association/American Stroke Association. ICH=intracerebral haemorrhage. PAIS=Paracetamol
140 mm Hg is safe and might reduce the risk of HE in
(Acetaminophen) In Stroke. The level of evidence is according to the Oxford Centre for Evidence-based Medicine (Level 1A
being the highest level of evidence).64 patients treated within 6 h of onset of ICH, but had no
effect on outcome.20,46 In ATACH, aggressive SBP
reduction to 110–140 mm Hg in the first 24 h was well
outcomes,12,177 although the optimum glucose target and tolerated, with a low risk of HE, neurological deterioration,
duration of glucose control in patients with ICH are and in-hospital mortality.47
unclear. However, studies have suggested targeting a The results of both INTERACT 2 and ATACH 2 are
glucose concentration of 150 mg/dL in the acute setting of awaited, and might further answer the question of
ICH,12,174 and the avoidance of hyperglycaemia during the whether there are other benefits of early SBP reduction
first 72 h after symptom onset, possibly because admission in patients with ICH, and provide clearer evidence for
hyperglycaemia can persist for at least 72 h post ictus.174,177 the target BP and the choice of drugs. Pending these
Although large RCTs are needed to define the optimum results, the AHA/ASA guidelines recommend BP
glucose target and duration of treatment that can improve lowering if SBP is 150–220 mm Hg or MAP is higher
clinical outcomes in patients with ICH, an increased than 150 mm Hg, and that acute lowering of SBP to
serum glucose of more than 140 mg/dL (>7·8 mmol/L) 140 mm Hg is probably safe.45 Meanwhile, the EUSI
should be treated with insulin.2,45 recommends a target of 160/100 mm Hg or a MAP of
125 mm Hg in patients with a history of hypertension
Increased blood pressure and 150/90 mm Hg or a MAP of 110 mm Hg in those
Clinical features without a history of hypertension.64
Increased BP (≥140/90 mm Hg) is common in the acute
phase of ICH, occurring in more than 70% of patients on Conclusions
presentation.180,181 Increased BP in the acute setting of Complications occurring during the acute phase of ICH
ICH occurs even in the absence of a previous history of add further detrimental effects to an already potentially
hypertension and is independently associated with poor fatal disorder and substantially affect the clinical
outcome.180,182 outcome. In view of the small number of therapeutic
The mechanism for the acute increase of BP after options available for ICH, a need exists to provide the
ICH is unknown. However, it is proposed to be a best evidence-based supportive care. Patients should be
112 www.thelancet.com/neurology Vol 11 January 2012
Review
managed in a neuroscience ICU or a similar setting managed on the basis of current recommendations and
during the acute phase of ICH, with continuous guidelines, especially when little evidence exists or
monitoring of vital signs and frequent neurological when trials are still in progress. Once patients are
assessment. Improved surveillance is needed for the stabilised, early rehabilitation is needed to prevent or
early detection of complications, which should be reduce the risk of further complications. The
Description Level of evidence*
General Data from the post-hoc analysis of the ATACH trial has linked a decrease in serum glucose concentration to a Level 1B
considerations reduction in haematoma expansion and improved clinical outcome177
Optimum The optimum glucose target is unclear and various glucose concentrations from 127 mg/dL to 180 mg/dL have been Level 1B
glucose target suggested; some prospective studies have suggested a target glucose concentration of 150 mg/dL in the acute
setting of ICH12,174
In the Oxfordshire Community Stroke Project, in 645 patients (86%) with ischaemic stroke and 105 (14%) with Level 2B
haemorrhagic stroke, a plasma glucose concentration higher than 144 mg/dL (>8 mmol/L) was associated with
increased mortality, particularly in the first month after stroke178
In the Acute Brain Bleeding Analysis, a prospective study of 1387 patients with ICH, an admission glucose Level 1B
concentration of >167 mg/dL was shown to be an independent risk factor for early mortality176
Optimum The optimum duration of glucose control is unclear, although studies have suggested the avoidance of hyperglycaemia ··
duration of during the first 72 h of symptom onset, possibly because admission hyperglycaemia can persist for up to 72 h post ictus174,177
glucose control In a post-hoc analysis of the ATACH trial, patients who had serum glucose reduction during the first 72 h after ICH had Level 1B
a lower relative risk of death or disability at 3 months177
In a prospective observational study of 295 patients, individuals with a serum glucose concentration maintained Level 1B
within 60–150 mg/dL during the first 72 h after ICH did better than those with a persistently high serum glucose
concentration174
In GIST-UK, which had a shorter duration than did ATACH, 24 h of intensive glucose control did not reduce mortality Level 2B
or improve functional outcome in the treatment group,179 although the trial had a small number of patients with ICH
(114 of the total 933) randomly allocated to treatment within 24 h of stroke onset; no separate analysis for patients
with ICH was reported
AHA/ASA guidelines suggest that serum glucose concentrations of >140 mg/dL (>7·8 mmol/L) should be treated Level 2a C
with insulin2,45
AHA/ASA=American Heart Association/American Stroke Association. ATACH=Antihypertensive Treatment of Acute Cerebral Hemorrhage. GIST-UK=UK Glucose Insulin in Stroke
Trial. ICH=intracerebral haemorrhage. *The level of evidence is according to the Oxford Centre for Evidence-based Medicine (Level 1A being the highest level of evidence).64
Table 7: Clinical management of hyperglycaemia after intracerebral haemorrhage
Description Level of evidence*
Blood pressure control The INTERACT pilot trial that compared intensive (target SBP 140 mm Hg) with guideline-based (target SBP 180 mm Hg) BP control showed the Level 1B
feasibility and safety of early intensive BP reduction within the first 6 h of onset of supratentorial ICH; however, no statistically significant
difference was recorded in functional outcome at 3 months between the two groups (median mRS score was 2 in both groups; p=0·66)20
In the ATACH phase 1 trial, patients with a SBP of >170 mm Hg were treated with intravenous nicardipine within 6 h of onset of lobar Level 1B
supratentorial ICH to reduce BP in three escalating target BP tiers: tier 1 (170–200 mm Hg; n=18), tier 2 (140–170 mm Hg; n=20), and tier 3
(110–140 mm Hg; n=22); BP reduction was safe and feasible in all three tiers 47
AHA/ASA guidelines recommend that in patients presenting with a SBP of 150–220 mm Hg, acute lowering of SBP to 140 mm Hg is Level 2a B
probably safe45
Target blood pressure The following target BP should be considered in various situations:2,45
If SBP is >200 mm Hg or MAP is >150 mm Hg, aggressive reduction of BP could be considered with continuous intravenous infusion, with Level 2b C
frequent BP monitoring every 5 min
If SBP is >180 mm Hg or MAP is >130 mm Hg and there is the possibility of increased ICP, then consider monitoring ICP and reducing BP using
intermittent or continuous intravenous drugs while maintaining a cerebral perfusion pressure of 60 mm Hg
If SBP is >180 mm Hg or MAP is >130 mm Hg and there is no evidence of increased ICP, then consider a slight reduction of BP (eg, MAP of
110 mm Hg or target BP of 160/90 mm Hg), using intermittent or continuous intravenous drugs to control BP, and clinically re-examine the
patient every 15 min
If SBP exceeds 180 mm Hg or MAP exceeds 130 mm Hg, management should involve either bolus or continuous infusion of drugs to a target Level 2b C
MAP of 110 mm Hg or less or a goal BP of 160/90 mm Hg
Antihypertensive Suitable antihypertensive drugs include labetalol, esmolol, or nicardipine (drugs with a cerebral vasodilation effect should be avoided)2 Level 2bC
drugs recommended Labetalol: 5–20 mg (intermittent boluses) every 15 min or 2 mg/min in continuous infusion (drip)
in AHA/ASA guidelines Esmolol: 250 mcg/kg (loading dose), then 25–300 mcg/kg per min (maintenance)
Nicardipine: 5–15 mg/h
Hydralazine: 5–20 mg (intermittent boluses)
Nitroprusside: 0·1–10 mcg/kg per min
AHA/ASA=American Heart Association/American Stroke Association. ATACH=Antihypertensive Treatment of Acute Cerebral Haemorrhage. BP=blood pressure. ICH=intracerebral haemorrhage. ICP=intracranial
pressure. INTERACT=Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial. MAP=mean arterial pressure. mRS=modified Rankin score. SBP=systolic blood pressure. *The level of evidence is
according to the Oxford Centre for Evidence-based Medicine (Level 1A being the highest level of evidence).64
Table 8: Clinical management of raised blood pressure after intracerebral haemorrhage
www.thelancet.com/neurology Vol 11 January 2012 113
Review
7 Brott T, Broderick J, Kothari R, et al. Early hemorrhage growth in
Search strategy and selection criteria patients with intracerebral hemorrhage. Stroke 1997; 28: 1–5.
8 Mayer SA, Brun NC, Begtrup K, et al, and the Recombinant
We searched Medline and the Cochrane Library, reference lists Activated Factor VII Intracerebral Hemorrhage Trial Investigators.
of retrieved articles, and main journal contents pages, and we Recombinant activated factor VII for acute intracerebral
hemorrhage. N Engl J Med 2005; 352: 777–85.
also did cross referencing. Search terms included 9 Tuhrim S, Horowitz DR, Sacher M, Godbold JH. Volume of
“h(a)emorrhagic stroke”, “cerebral h(a)emorrhage”, ventricular blood is an important determinant of outcome in
“intracerebral h(a)emorrhage”, “primary intracerebral h(a) supratentorial intracerebral hemorrhage. Crit Care Med 1999;
27: 617–21.
emorrhage”, “spontaneous intracerebral h(a)emorrhage”, 10 Bhattathiri PS, Gregson B, Prasad KS, Mendelow AD, and the
“complications”, “neurological complications”, “medical STICH Investigators. Intraventricular hemorrhage and
complications”, “management”, “treatment”, and “outcome”. hydrocephalus after spontaneous intracerebral hemorrhage: results
from the STICH trial. Acta Neurochir Suppl (Wien) 2006; 96: 65–8.
The search included both human and animal studies, and was 11 Steiner T, Diringer MN, Schneider D, et al. Dynamics of
restricted to studies published in English before November, intraventricular hemorrhage in patients with spontaneous
2011. Studies were selected on the basis of relevance to the intracerebral hemorrhage: risk factors, clinical impact, and effect of
hemostatic therapy with recombinant activated factor VII.
topics covered in the Review. Guidelines for the management Neurosurgery 2006; 59: 767–73.
of acute ischaemic stroke and intracerebral haemorrhage 12 Kimura K, Iguchi Y, Inoue T, et al. Hyperglycemia independently
from the American Heart Association and the European increases the risk of early death in acute spontaneous intracerebral
hemorrhage. J Neurol Sci 2007; 255: 90–94.
Stroke Organisation were also reviewed.
13 Fogelholm R, Murros K, Rissanen A, Avikainen S. Admission blood
glucose and short term survival in primary intracerebral
haemorrhage: a population based study.
implementation of appropriate preventative and thera- J Neurol Neurosurg Psychiatry 2005; 76: 349–53.
peutic interventions could minimise the morbidity and 14 Mayer SA, Sacco RL, Shi T, Mohr JP. Neurologic deterioration in
noncomatose patients with supratentorial intracerebral
mortality associated with this devastating type of hemorrhage. Neurology 1994; 44: 1379–84.
stroke. A clear need exists for further research into the 15 Kumar S, Selim MH, Caplan LR. Medical complications after
prevention and treatment of ICH complications to stroke. Lancet Neurol 2010; 9: 105–18.
improve the level of evidence available, because most 16 Balami JS, Chen RL, Grunwald IQ, Buchan AM. Neurological
complications of acute ischaemic stroke. Lancet Neurol 2011;
guidelines and recommendations are based on 10: 357–71.
empirical data. 17 Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T.
Enlargement of spontaneous intracerebral hemorrhage. Incidence
Contributors and time course. Stroke 1996; 27: 1783–87.
JSB searched the literature, reviewed available studies, and wrote the
18 Fujitsu K, Muramoto M, Ikeda Y, Inada Y, Kim I, Kuwabara T.
paper. AMB reviewed and made critical revisions of the paper. Indications for surgical treatment of putaminal hemorrhage.
Conflicts of interest Comparative study based on serial CT and time-course analysis.
We declare that we have no conflicts of interest. J Neurosurg 1990; 73: 518–25.
19 Fujii Y, Takeuchi S, Sasaki O, Minakawa T, Tanaka R. Multivariate
Acknowledgments analysis of predictors of hematoma enlargement in spontaneous
We are grateful for funding received from the Biomedical Research intracerebral hemorrhage. Stroke 1998; 29: 1160–66.
Centre, the Fondation Leducq, the Dunhill Medical Trust, the Henry 20 Anderson CS, Huang Y, Wang JG, et al, and the INTERACT
Smith Charity, and the Oxford University Hospitals NHS Trust, UK. Investigators. Intensive Blood Pressure Reduction in Acute Cerebral
Haemorrhage Trial (INTERACT): a randomised pilot trial.
References
Lancet Neurol 2008; 7: 391–99.
1 Broderick JP, Brott T, Tomsick T, Miller R, Huster G. Intracerebral
hemorrhage more than twice as common as subarachnoid 21 Silva Y, Leira R, Tejada J, Lainez JM, Castillo J, Dávalos A, and the
hemorrhage. J Neurosurg 1993; 78: 188–91. Stroke Project, Cerebrovascular Diseases Group of the Spanish
Neurological Society. Molecular signatures of vascular injury are
2 Broderick J, Connolly S, Feldmann E, et al, and the American Heart
associated with early growth of intracerebral hemorrhage. Stroke
Association, and the American Stroke Association Stroke Council,
2005; 36: 86–91.
and the High Blood Pressure Research Council, and the Quality of
Care and Outcomes in Research Interdisciplinary Working Group. 22 Mayer SA. Ultra-early hemostatic therapy for intracerebral
Guidelines for the management of spontaneous intracerebral hemorrhage. Stroke 2003; 34: 224–29.
hemorrhage in adults: 2007 update: a guideline from the American 23 Davis SM, Broderick J, Hennerici M, et al, and the Recombinant
Heart Association/American Stroke Association Stroke Council, Activated Factor VII Intracerebral Hemorrhage Trial Investigators.
High Blood Pressure Research Council, and the Quality of Care and Hematoma growth is a determinant of mortality and poor outcome
Outcomes in Research Interdisciplinary Working Group. Stroke after intracerebral hemorrhage. Neurology 2006; 66: 1175–81.
2007; 38: 2001–23. 24 Flibotte JJ, Hagan N, O’Donnell J, Greenberg SM, Rosand J.
3 Counsell C, Boonyakarnkul S, Dennis M, et al. Primary Warfarin, hematoma expansion, and outcome of intracerebral
intracerebral haemorrhage in the Oxfordshire Community Stroke hemorrhage. Neurology 2004; 63: 1059–64.
Project, 2: prognosis. Cerebrovasc Dis 1995; 5: 26–34. 25 Cucchiara B, Messe S, Sansing L, Kasner S, Lyden P, and the
4 Sacco S, Marini C, Toni D, Olivieri L, Carolei A. Incidence and CHANT Investigators. Hematoma growth in oral anticoagulant
10-year survival of intracerebral hemorrhage in a population-based related intracerebral hemorrhage. Stroke 2008; 39: 2993–96.
registry. Stroke 2009; 40: 394–99. 26 Huttner HB, Schellinger PD, Hartmann M, et al. Hematoma
5 Zia E, Engström G, Svensson PJ, Norrving B, Pessah-Rasmussen H. growth and outcome in treated neurocritical care patients with
Three-year survival and stroke recurrence rates in patients with intracerebral hemorrhage related to oral anticoagulant therapy:
primary intracerebral hemorrhage. Stroke 2009; 40: 3567–73. comparison of acute treatment strategies using vitamin K, fresh
6 van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, frozen plasma, and prothrombin complex concentrates. Stroke
Klijn CJ. Incidence, case fatality, and functional outcome of 2006; 37: 1465–70.
intracerebral haemorrhage over time, according to age, sex, and 27 Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM.
ethnic origin: a systematic review and meta-analysis. Lancet Neurol The effect of warfarin and intensity of anticoagulation on outcome
2010; 9: 167–76. of intracerebral hemorrhage. Arch Intern Med 2004; 164: 880–84.
114 www.thelancet.com/neurology Vol 11 January 2012
Review
28 Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” 47 Qureshi AI, Tariq N, Divani AA, et al, and the Antihypertensive
predicts hematoma expansion in acute intracerebral hemorrhage. Treatment of Acute Cerebral Hemorrhage (ATACH) investigators.
Stroke 2007; 38: 1257–62. Antihypertensive treatment of acute cerebral hemorrhage.
29 Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on Crit Care Med 2010; 38: 637–48.
CT angiography predicts hematoma expansion in intracerebral 48 Prasad K, Mendelow AD, Gregson B. Surgery for Primary
hemorrhage. Neurology 2007; 68: 889–94. Supratentorial Intracerbral Haemorrhage (Review) in: The
30 Kim J, Smith A, Hemphill JC 3rd, et al. Contrast extravasation on Cochrane Library 2009 Issue 1, Chichester. UK: John Wiley &
CT predicts mortality in primary intracerebral hemorrhage. Sons Ltd.
AJNR Am J Neuroradiol 2008; 29: 520–25. 49 Mendelow AD, Gregson BA, Fernandes HM, et al, and the STICH
31 Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. The spot sign investigators. Early surgery versus initial conservative treatment in
score in primary intracerebral hemorrhage identifies patients at patients with spontaneous supratentorial intracerebral haematomas
highest risk of in-hospital mortality and poor outcome among in the International Surgical Trial in Intracerebral Haemorrhage
survivors. Stroke 2010; 41: 54–60. (STICH): a randomised trial. Lancet 2005; 365: 387–97.
32 Broderick JP, Diringer MN, Hill MD, et al, and the Recombinant 50 Murthy JM, Chowdary GV, Murthy TV, Bhasha PS, Naryanan TJ.
Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Decompressive craniectomy with clot evacuation in large
Determinants of intracerebral hemorrhage growth: an exploratory hemispheric hypertensive intracerebral hemorrhage. Neurocrit Care
analysis. Stroke 2007; 38: 1072–75. 2005; 2: 258–62.
33 Barras CD, Tress BM, Christensen S, et al, and the Recombinant 51 Ramnarayan R, Anto D, Anilkumar TV, Nayar R. Decompressive
Activated Factor VII Intracerebral Hemorrhage Trial Investigators. hemicraniectomy in large putaminal hematomas: an Indian
Density and shape as CT predictors of intracerebral hemorrhage experience. J Stroke Cerebrovasc Dis 2009; 18: 1–10.
growth. Stroke 2009; 40: 1325–31. 52 Vespa P, McArthur D, Miller C, et al. Frameless stereotactic
34 Naidech AM, Jovanovic B, Liebling S, et al. Reduced platelet aspiration and thrombolysis of deep intracerebral hemorrhage is
activity is associated with early clot growth and worse 3-month associated with reduction of hemorrhage volume and neurological
outcome after intracerebral hemorrhage. Stroke 2009; improvement. Neurocrit Care 2005; 2: 274–81.
40: 2398–401. 53 Carhuapoma JR, Barrett RJ, Keyl PM, Hanley DF, Johnson RR.
35 Delgado P, Alvarez-Sabín J, Abilleira S, et al. Plasma D-dimer Stereotactic aspiration-thrombolysis of intracerebral hemorrhage
predicts poor outcome after acute intracerebral hemorrhage. and its impact on perihematoma brain edema. Neurocrit Care 2008;
Neurology 2006; 67: 94–98. 8: 322–29.
36 Kazui S, Minematsu K, Yamamoto H, Sawada T, Yamaguchi T. 54 Zuccarello M, Brott T, Derex L, et al. Early surgical treatment for
Predisposing factors to enlargement of spontaneous intracerebral supratentorial intracerebral hemorrhage: a randomized feasibility
hematoma. Stroke 1997; 28: 2370–75. study. Stroke 1999; 30: 1833–39.
37 Ohwaki K, Yano E, Nagashima H, Hirata M, Nakagomi T, 55 Teernstra OPM, Evers SMAA, Lodder J, Leffers P, Franke CL,
Tamura A. Blood pressure management in acute intracerebral Blaauw G. Stereotactic treatment of intracerebral hematoma by
hemorrhage: relationship between elevated blood pressure and means of a plasminogen activator: a multicenter randomized
hematoma enlargement. Stroke 2004; 35: 1364–67. controlled trial (SICHPA). Stroke 2003; 34: 968–74.
38 Martí-Fàbregas J, Martínez-Ramírez S, Martínez-Corral M, et al. 56 Wang WZ, Jiang B, Liu HM, et al. Minimally invasive
Blood pressure is not associated with haematoma enlargement craniopuncture therapy vs. conservative treatment for spontaneous
in acute intracerebral haemorrhage. Eur J Neurol 2008; intracerebral hemorrhage: results from a randomized clinical trial
15: 1085–90. in China. Int J Stroke 2009; 4: 11–16.
39 Creutzfeldt CJ, Weinstein JR, Longstreth WT Jr, Becker KJ, 57 Sun H, Liu H, Li D, Liu L, Yang J, Wang W. An effective treatment for
McPharlin TO, Tirschwell DL. Prior antiplatelet therapy, platelet cerebral hemorrhage: minimally invasive craniopuncture combined
infusion therapy, and outcome after intracerebral hemorrhage. with urokinase infusion therapy. Neurol Res 2010; 32: 371–77.
J Stroke Cerebrovasc Dis 2009; 18: 221–28. 58 Zhou H, Zhang Y, Liu L, et al. Minimally invasive stereotactic
40 Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, puncture and thrombolysis therapy improves long-term outcome after
Kasner SE, and the CHANT Investigators. Prior antiplatelet use acute intracerebral hemorrhage. J Neurol 2011; 258: 661–69.
does not affect hemorrhage growth or outcome after ICH. 59 Auer LM, Ascher PW, Heppner F, et al. Does acute endoscopic
Neurology 2009; 72: 1397–402. evacuation improve the outcome of patients with spontaneous
41 Caso V, Paciaroni M, Venti M, et al. Effect of on-admission intracerebral hemorrhage? Eur Neurol 1985; 24: 254–61.
antiplatelet treatment on patients with cerebral hemorrhage. 60 Miller CM, Vespa P, Saver JL, et al. Image-guided endoscopic
Cerebrovasc Dis 2007; 24: 215–18. evacuation of spontaneous intracerebral hemorrhage. Surg Neurol
42 Rodriguez-Luna D, Rubiera M, Ribo M, et al. Ultraearly 2008; 69: 441–46, discussion 446.
hematoma growth predicts poor outcome after acute intracerebral 61 Barlas O, Karadereler S, Bahar S, et al. Image-guided keyhole
hemorrhage. Neurology 2011; 77: 1599–604. evacuation of spontaneous supratentorial intracerebral hemorrhage.
43 Mayer SA, Brun NC, Begtrup K, et al, and the FAST Trial Minim Invasive Neurosurg 2009; 52: 62–68.
Investigators. Efficacy and safety of recombinant activated factor 62 Chen CC, Lin HL, Cho DY. Endoscopic surgery for thalamic
VII for acute intracerebral hemorrhage. N Engl J Med 2008; hemorrhage: a technical note. Surg Neurol 2007; 68: 438–42,
358: 2127–37. discussion 442.
44 Mayer SA, Davis SM, Skolnick BE, et al, and the FAST trial 63 Nishihara T, Nagata K, Tanaka S, et al. Newly developed endoscopic
investigators. Can a subset of intracerebral hemorrhage patients instruments for the removal of intracerebral hematoma.
benefit from hemostatic therapy with recombinant activated factor Neurocrit Care 2005; 2: 67–74.
VII? Stroke 2009; 40: 833–40. 64 Oxford Centre for Evidence-based Medicine Level of Evidence.
45 Morgenstern LB, Hemphill JC 3rd, Anderson C, et al, and the http://www.cebm.net (accessed October 26, 2011).
American Heart Association Stroke Council and Council on 65 Yuan ZH, Jiang JK, Huang WD, Pan J, Zhu JY, Wang JZ.
Cardiovascular Nursing. Guidelines for the management of A meta-analysis of the efficacy and safety of recombinant activated
spontaneous intracerebral hemorrhage: a guideline for healthcare factor VII for patients with acute intracerebral hemorrhage without
professionals from the American Heart Association/American hemophilia. J Clin Neurosci 2010; 17: 685–93.
Stroke Association. Stroke 2010; 41: 2108–29; published online 66 Morgan T, Zuccarello M, Nrayan R, et al. Preliminary findings of
July 22, 2010. the Minimally Invasive Surgery plus rtPA for Intracerabral
46 Anderson CS, Huang Y, Arima H, et al, and the INTERACT Haemorrhage Evacuation (MISTIE) clinical trial.
Investigators. Effects of early intensive blood pressure-lowering Acta Neurochir Suppl (Wien) 2008; 105: 147–51.
treatment on the growth of hematoma and perihematomal edema 67 Majeed A, Kim YK, Roberts RS, Holmström M, Schulman S.
in acute intracerebral hemorrhage: the Intensive Blood Pressure Optimal timing of resumption of warfarin after intracranial
Reduction in Acute Cerebral Haemorrhage Trial (INTERACT). hemorrhage. Stroke 2010; 41: 2860–66.
Stroke 2010; 41: 307–12.
www.thelancet.com/neurology Vol 11 January 2012 115
Review
68 Hawryluk GW, Austin JW, Furlan JC, Lee JB, O’Kelly C, 90 Vemmos KN, Tsivgoulis G, Spengos K, et al. Association between
Fehlings MG. Management of anticoagulation following central 24-h blood pressure monitoring variables and brain oedema in
nervous system hemorrhage in patients with high thromboembolic patients with hyperacute stroke. J Hypertens 2003; 21: 2167–73.
risk. J Thromb Haemost 2010; 8: 1500–08. 91 Schellinger PD, Fiebach JB, Hoffmann K, et al. Stroke MRI in
69 Romualdi E, Micieli E, Ageno W, Squizzato A. Oral anticoagulant intracerebral hemorrhage: is there a perihemorrhagic penumbra?
therapy in patients with mechanical heart valve and intracranial Stroke 2003; 34: 1674–79.
haemorrhage. A systematic review. Thromb Haemost 2009; 92 Herweh C, Jüttler E, Schellinger PD, et al. Evidence against a
101: 290–97. perihemorrhagic penumbra provided by perfusion computed
70 Steiner T, Kaste M, Forsting M, et al. Recommendations for the tomography. Stroke 2007; 38: 2941–47.
management of intracranial haemorrhage—Part I: spontaneous 93 Bratton SL, Chestnut RM, Ghajar J, et al, and the Brain Trauma
intracerebral haemorrhage. The European Stroke Initiative Writing Foundation, and the American Association of Neurological
Committee and the Writing Committee for the EUSI Executive Surgeons, and the Congress of Neurological Surgeons, and the Joint
Committee. Cerebrovasc Dis 2006; 22: 294–316. Section on Neurotrauma and Critical Care, AANS/CNS. Guidelines
71 Hankey GJ, Eikelboom JW. Antithrombotic drugs for patients with for the management of severe traumatic brain injury. IX. Cerebral
ischaemic stroke and transient ischaemic attack to prevent perfusion thresholds. J Neurotrauma 2007; 24 (suppl 1): S59–64.
recurrent major vascular events. Lancet Neurol 2010; 9: 273–84. 94 Kollmar R, Staykov D, Dörfler A, Schellinger PD, Schwab S,
72 Schulman S, Kearon C, Kakkar AK, et al, and the RE-COVER Study Bardutzky J. Hypothermia reduces perihemorrhagic edema after
Group. Dabigatran versus warfarin in the treatment of acute venous intracerebral hemorrhage. Stroke 2010; 41: 1684–89.
thromboembolism. N Engl J Med 2009; 361: 2342–52. 95 Hallevi H, Albright KC, Aronowski J, et al. Intraventricular
73 Zazulia AR, Diringer MN, Derdeyn CP, Powers WJ. Progression of hemorrhage: Anatomic relationships and clinical implications.
mass effect after intracerebral hemorrhage. Stroke 1999; 30: 1167–73. Neurology 2008; 70: 848–52.
74 Inaji M, Tomita H, Tone O, Tamaki M, Suzuki R, Ohno K. 96 Hanley DF. Intraventricular hemorrhage: severity factor and
Chronological changes of perihematomal edema of human treatment target in spontaneous intracerebral hemorrhage.
intracerebral hematoma. Acta Neurochir Suppl (Wien) 2003; Stroke 2009; 40: 1533–38.
86: 445–48. 97 Staykov D, Huttner HB, Struffert T, et al. Intraventricular
75 Gebel JM Jr, Jauch EC, Brott TG, et al. Relative edema volume is a fibrinolysis and lumbar drainage for ventricular hemorrhage.
predictor of outcome in patients with hyperacute spontaneous Stroke 2009; 40: 3275–80.
intracerebral hemorrhage. Stroke 2002; 33: 2636–41. 98 Young WB, Lee KP, Pessin MS, Kwan ES, Rand WM, Caplan LR.
76 Butcher KS, Baird T, MacGregor L, Desmond P, Tress B, Davis S. Prognostic significance of ventricular blood in supratentorial
Perihematomal edema in primary intracerebral hemorrhage is hemorrhage: a volumetric study. Neurology 1990; 40: 616–19.
plasma derived. Stroke 2004; 35: 1879–85. 99 Hemphill JC 3rd, Bonovich DC, Besmertis L, Manley GT,
77 Rincon F, Mayer SA. Novel therapies for intracerebral hemorrhage. Johnston SC. The ICH score: a simple, reliable grading scale for
Curr Opin Crit Care 2004; 10: 94–100. intracerebral hemorrhage. Stroke 2001; 32: 891–97.
78 Wagner KR, Sharp FR, Ardizzone TD, Lu A, Clark JF. Heme and 100 Adams RE, Diringer MN. Response to external ventricular drainage
iron metabolism: role in cerebral hemorrhage. in spontaneous intracerebral hemorrhage with hydrocephalus.
J Cereb Blood Flow Metab 2003; 23: 629–52. Neurology 1998; 50: 519–23.
79 Lee KR, Kawai N, Kim S, Sagher O, Hoff JT. Mechanisms of edema 101 Hanley DF, Naff NJ, Harris DM. Intraventricular hemorrhage:
formation after intracerebral hemorrhage: effects of thrombin on Presentations and management options.
cerebral blood flow, blood-brain barrier permeability, and cell Semin Cerebrovasc Dis Stroke 2005; 5: 209–16.
survival in a rat model. J Neurosurg 1997; 86: 272–78. 102 Wasserman JK, Zhu X, Schlichter LC. Evolution of the
80 Xi G, Keep RF, Hoff JT. Mechanisms of brain injury after inflammatory response in the brain following intracerebral
intracerebral haemorrhage. Lancet Neurol 2006; 5: 53–63. hemorrhage and effects of delayed minocycline treatment.
81 Thiex R, Tsirka SE. Brain edema after intracerebral hemorrhage: Brain Res 2007; 1180: 140–54.
mechanisms, treatment options, management strategies, and 103 Zhao X, Zhang Y, Strong R, Zhang J, Grotta JC, Aronowski J.
operative indications. Neurosurg Focus 2007; 22: E6. Distinct patterns of intracerebral hemorrhage-induced alterations in
82 Xi G, Wagner KR, Keep RF, et al. Role of blood clot formation on NF-kappaB subunit, iNOS, and COX-2 expression. J Neurochem
early edema development after experimental intracerebral 2007; 101: 652–63.
hemorrhage. Stroke 1998; 29: 2580–86. 104 Hallevi H, Dar NS, Barreto AD, et al. The IVH score: a novel tool
83 Makogonenko E, Tsurupa G, Ingham K, Medved L. Interaction of for estimating intraventricular hemorrhage volume: clinical and
fibrin(ogen) with fibronectin: further characterization and localization research implications. Crit Care Med 2009; 37: 969–74, e1.
of the fibronectin-binding site. Biochemistry 2002; 41: 7907–13. 105 Diringer MN, Edwards DF, Zazulia AR. Hydrocephalus:
84 Arima H, Wang JG, Huang Y, et al, and the INTERACT a previously unrecognized predictor of poor outcome from
Investigators. Significance of perihematomal edema in acute supratentorial intracerebral hemorrhage. Stroke 1998; 29: 1352–57.
intracerebral hemorrhage: the INTERACT trial. Neurology 2009; 106 Naff NJ, Carhuapoma JR, Williams MA, et al. Treatment of
73: 1963–68. intraventricular hemorrhage with urokinase: effects on 30-day
85 Mehdiratta M, Kumar S, Hackney D, Schlaug G, Selim M. survival. Stroke 2000; 31: 841–47.
Association between serum ferritin level and perihematoma edema 107 Huttner HB, Nagel S, Tognoni E, et al. Intracerebral hemorrhage
volume in patients with spontaneous intracerebral hemorrhage. with severe ventricular involvement: lumbar drainage for
Stroke 2008; 39: 1165–70. communicating hydrocephalus. Stroke 2007; 38: 183–87.
86 Venkatasubramanian C, Mlynash M, Finley-Caulfield A, et al. 108 Sumer MM, Açikgöz B, Akpinar G. External ventricular drainage
Natural history of perihematomal edema after intracerebral for acute obstructive hydrocephalus developing following
hemorrhage measured by serial magnetic resonance imaging. spontaneous intracerebral haemorrhages. Neurol Sci 2002;
Stroke 2011; 42: 73–80. 23: 29–33.
87 Carhuapoma JR, Hanley DF, Banerjee M, Beauchamp NJ. Brain 109 Naff NJ, Hanley DF, Keyl PM, et al. Intraventricular thrombolysis
edema after human cerebral hemorrhage: a magnetic resonance speeds blood clot resolution: results of a pilot, prospective,
imaging volumetric analysis. J Neurosurg Anesthesiol 2003; randomized, double-blind, controlled trial. Neurosurgery 2004;
15: 230–33. 54: 577–83, discussion 583.
88 Castillo J, Dávalos A, Alvarez-Sabín J, et al. Molecular signatures of 110 Huttner HB, Tognoni E, Bardutzky J, et al. Influence of
brain injury after intracerebral hemorrhage. Neurology 2002; intraventricular fibrinolytic therapy with rt-PA on the long-term
58: 624–29. outcome of treated patients with spontaneous basal ganglia
89 Abilleira S, Montaner J, Molina CA, Monasterio J, Castillo J, hemorrhage: a case-control study. Eur J Neurol 2008; 15: 342–49.
Alvarez-Sabín J. Matrix metalloproteinase-9 concentration after 111 Fountas KN, Kapsalaki EZ, Parish DC, et al. Intraventricular
spontaneous intracerebral hemorrhage. J Neurosurg 2003; administration of rt-PA in patients with intraventricular
99: 65–70. hemorrhage. South Med J 2005; 98: 767–73.
116 www.thelancet.com/neurology Vol 11 January 2012
Review
112 Rohde V, Schaller C, Hassler WE. Intraventricular recombinant 136 Naidech AM, Garg RK, Liebling S, et al. Anticonvulsant use and
tissue plasminogen activator for lysis of intraventricular outcomes after intracerebral hemorrhage. Stroke 2009;
haemorrhage. J Neurol Neurosurg Psychiatry 1995; 58: 447–51. 40: 3810–15.
113 Wong GK, Poon WS, Wai S, Yu LM, Lyon D, Lam JM. Failure of 137 Messé SR, Sansing LH, Cucchiara BL, Herman ST, Lyden PD,
regular external ventricular drain exchange to reduce cerebrospinal Kasner SE, and the CHANT investigators. Prophylactic antiepileptic
fluid infection: result of a randomised controlled trial. drug use is associated with poor outcome following ICH.
J Neurol Neurosurg Psychiatry 2002; 73: 759–61. Neurocrit Care 2009; 11: 38–44.
114 Lozier AP, Sciacca RR, Romagnoli MF, Connolly ES Jr. 138 Goldstein JN, Fazen LE, Wendell L, et al. Risk of thromboembolism
Ventriculostomy-related infections: a critical review of the literature. following acute intracerebral hemorrhage. Neurocrit Care 2009;
Neurosurgery 2002; 51: 170–81, discussion 181–82. 10: 28–34.
115 Andrews CO, Engelhard HH. Fibrinolytic therapy in 139 Gregory PC, Kuhlemeier KV. Prevalence of venous
intraventricular hemorrhage. Ann Pharmacother 2001; 35: 1435–48. thromboembolism in acute hemorrhagic and thromboembolic
116 Nieuwkamp DJ, de Gans K, Rinkel GJ, Algra A. Treatment and stroke. Am J Phys Med Rehabil 2003; 82: 364–69.
outcome of severe intraventricular extension in patients with 140 Tetri S, Hakala J, Juvela S, et al. Safety of low-dose subcutaneous
subarachnoid or intracerebral hemorrhage: a systematic review of enoxaparin for the prevention of venous thromboembolism after
the literature. J Neurol 2000; 247: 117–21. primary intracerebral haemorrhage. Thromb Res 2008;
117 Morgan T, Awad I, Keyl P, Lane K, Hanley D. Preliminary report of 123: 206–12.
the Clot Lysis Evaluating Accelerated Resolution of Intraventricular 141 Kim KS, Brophy GM. Symptomatic venous thromboembolism:
Hemorrhage (CLEAR-IVH) clinical trial. incidence and risk factors in patients with spontaneous or
Acta Neurochir Suppl (Wien) 2008; 105: 217–20. traumatic intracranial hemorrhage. Neurocrit Care 2009;
118 Longatti PL, Martinuzzi A, Fiorindi A, Maistrello L, Carteri A. 11: 28–33.
Neuroendoscopic management of intraventricular hemorrhage. 142 Lacut K, Bressollette L, Le Gal G, et al, and the VICTORIAh
Stroke 2004; 35: e35–38. (Venous Intermittent Compression and Thrombosis Occurrence
119 Zhang Z, Li X, Liu Y, Shao Y, Xu S, Yang Y. Application of Related to Intra-cerebral Acute hemorrhage) Investigators.
neuroendoscopy in the treatment of intraventricular hemorrhage. Prevention of venous thrombosis in patients with acute
Cerebrovasc Dis 2007; 24: 91–96. intracerebral hemorrhage. Neurology 2005; 65: 865–69.
120 Yadav YR, Mukerji G, Shenoy R, Basoor A, Jain G, Nelson A. 143 Ogata T, Yasaka M, Wakugawa Y, Inoue T, Ibayashi S, Okada Y.
Endoscopic management of hypertensive intraventricular Deep venous thrombosis after acute intracerebral hemorrhage.
haemorrhage with obstructive hydrocephalus. J Neurol Sci 2008; 272: 83–6.
BMC Neurol 2007; 7: 1. 144 Orken DN, Kenangil G, Ozkurt H, et al. Prevention of deep venous
121 Hamada H, Hayashi N, Kurimoto M, et al. Neuroendoscopic thrombosis and pulmonary embolism in patients with acute
removal of intraventricular hemorrhage combined with intracerebral hemorrhage. Neurologist 2009; 15: 329–31.
hydrocephalus. Minim Invasive Neurosurg 2008; 51: 345–49. 145 Zubkov AY, Wijdicks EF. Deep venous thrombosis prophylaxis in
122 Huttner HB, Schwab S, Bardutzky J. Lumbar drainage for cerebral hemorrhage. Rev Neurol Dis 2009; 6: 21–25.
communicating hydrocephalus after ICH with ventricular 146 Geerts WH, Bergqvist D, Pineo GF, et al, and the American College
hemorrhage. Neurocrit Care 2006; 5: 193–96. of Chest Physicians. Prevention of venous thromboembolism:
123 Passero S, Rocchi R, Rossi S, Ulivelli M, Vatti G. Seizures after American College of Chest Physicians Evidence-Based Clinical
spontaneous supratentorial intracerebral hemorrhage. Epilepsia Practice Guidelines (8th Edition). Chest 2008;
2002; 43: 1175–80. 133 (suppl): 381S–453S.
124 Bladin CF, Alexandrov AV, Bellavance A, et al. Seizures after stroke: 147 Christensen MC, Dawson J, Vincent C. Risk of thromboembolic
a prospective multicenter study. Arch Neurol 2000; 57: 1617–22. complications after intracerebral hemorrhage according to ethnicity.
125 Claassen J, Jetté N, Chum F, et al. Electrographic seizures and Adv Ther 2008; 25: 831–41.
periodic discharges after intracerebral hemorrhage. Neurology 2007; 148 Kawase K, Okazaki S, Toyoda K, et al. Sex difference in the
69: 1356–65. prevalence of deep-vein thrombosis in Japanese patients with acute
126 Vespa PM, O’Phelan K, Shah M, et al. Acute seizures after intracerebral hemorrhage. Cerebrovasc Dis 2009; 27: 313–19.
intracerebral hemorrhage: a factor in progressive midline shift and 149 Lukovits TG, Goddeau RP Jr. Critical care of patients with acute
outcome. Neurology 2003; 60: 1441–46. ischemic and hemorrhagic stroke: update on recent evidence and
127 Faught E, Peters D, Bartolucci A, Moore L, Miller PC. Seizures after international guidelines. Chest 2011; 139: 694–700.
primary intracerebral hemorrhage. Neurology 1989; 39: 1089–93. 150 Dennis M, Sandercock PA, Reid J, et al, and the CLOTS Trials
128 Szaflarski JP, Rackley AY, Kleindorfer DO, et al. Incidence of Collaboration. Effectiveness of thigh-length graduated compression
seizures in the acute phase of stroke: a population-based study. stockings to reduce the risk of deep vein thrombosis after stroke
Epilepsia 2008; 49: 974–81. (CLOTS trial 1): a multicentre, randomised controlled trial.
Lancet 2009; 373: 1958–65.
129 Kilpatrick CJ, Davis SM, Tress BM, Rossiter SC, Hopper JL,
Vandendriesen ML. Epileptic seizures in acute stroke. Arch Neurol 151 Boeer A, Voth E, Henze T, Prange HW. Early heparin therapy in
1990; 47: 157–60. patients with spontaneous intracerebral haemorrhage.
J Neurol Neurosurg Psychiatry 1991; 54: 466–67.
130 Sung CY, Chu NS. Epileptic seizures in intracerebral haemorrhage.
J Neurol Neurosurg Psychiatry 1989; 52: 1273–76. 152 Wasay M, Khan S, Zaki KS, et al. A non-randomized study of safety
and efficacy of heparin for DVT prophylaxis in intracerebral
131 Garrett MC, Komotar RJ, Starke RM, Merkow MB, Otten ML,
haemorrhage. J Pak Med Assoc 2008; 58: 362–64.
Connolly ES. Predictors of seizure onset after intracerebral
hemorrhage and the role of long-term antiepileptic therapy. 153 Decousus H, Leizorovicz A, Parent F, et al. Prevention du Risque
J Crit Care 2009; 24: 335–39. d’Embolie Pulmonaire par Interruption Cave Study Group. A
clinical trial of vena caval filters in the prevention of pulmonary
132 Bateman BT, Claassen J, Willey JZ, et al. Convulsive status
embolism in patients with proximal deep-vein thrombosis.
epilepticus after ischemic stroke and intracerebral hemorrhage:
N Engl J Med 1998; 338: 409–15.
frequency, predictors, and impact on outcome in a large
administrative dataset. Neurocrit Care 2007; 7: 187–93. 154 Kelly J, Hunt BJ, Lewis RR, Rudd A. Anticoagulation or inferior
vena cava filter placement for patients with primary intracerebral
133 De Reuck J, Hemelsoet D, Van Maele G. Seizures and epilepsy in
hemorrhage developing venous thromboembolism? Stroke 2003;
patients with a spontaneous intracerebral haematoma.
34: 2999–3005.
Clin Neurol Neurosurg 2007; 109: 501–04.
155 Young T, Tang H, Hughes R. Vena caval filters for the prevention of
134 Arboix A, García-Eroles L, Massons JB, Oliveres M, Comes E.
pulmonary embolism. Cochrane Database Syst Rev 2010;
Predictive factors of early seizures after acute cerebrovascular
2: CD006212.
disease. Stroke 1997; 28: 1590–94.
156 Somarouthu B, Yeddula K, Wicky S, Hirsch JA, Kalva SP. Long-term
135 Reith J, Jørgensen HS, Nakayama H, Raaschou HO, Olsen TS.
safety and effectiveness of inferior vena cava filters in patients with
Seizures in acute stroke: predictors and prognostic significance.
stroke. J Neurointerv Surg 2011; 3: 141–46.
The Copenhagen Stroke Study. Stroke 1997; 28: 1585–89.
www.thelancet.com/neurology Vol 11 January 2012 117
Review
157 Kalva SP, Wicky S, Waltman AC, Athanasoulis CA. TrapEase vena 171 Mayer SA, Kowalski RG, Presciutti M, et al. Clinical trial of a novel
cava filter: experience in 751 patients. J Endovasc Ther 2006; surface cooling system for fever control in neurocritical care
13: 365–72. patients. Crit Care Med 2004; 32: 2508–15.
158 Greenfield LJ, and the The PREPIC Study Group. The PREPIC 172 Hertog HM, Worp HB, Tseng MC, Dippel DW. Cooling therapy for
Study Group. Eight-year follow-up of patients with permanent vena acute stroke. Cochrane Database Syst Rev 2009; 21: 1.
cava filters in the prevention of pulmonary embolism: the PREPIC 173 Diringer MN, and the Neurocritical Care Fever Reduction Trial
(Prevention du Risque d’Embolie Pulmonaire par Interruption Group. Treatment of fever in the neurologic intensive care unit with
Cave) Randomized Study. Perspect Vasc Surg Endovasc Ther 2006; a catheter-based heat exchange system. Crit Care Med 2004;
18: 187–88. 32: 559–64.
159 Fukuda I, Fukui K, Minakawa M, Koyama M, Ichinoseki I, Suzuki Y. 174 Godoy DA, Piñero GR, Svampa S, Papa F, Di Napoli M.
Rescue surgical embolectomy for fatal pulmonary embolism in Hyperglycemia and short-term outcome in patients with
patient with intracranial hemorrhage. Ann Thorac Surg 2006; spontaneous intracerebral hemorrhage. Neurocrit Care 2008;
81: 735–37. 9: 217–29.
160 Eckman MH, Rosand J, Knudsen KA, Singer DE, Greenberg SM. 175 Stead LG, Jain A, Bellolio MF, et al. Emergency Department
Can patients be anticoagulated after intracerebral hemorrhage? hyperglycemia as a predictor of early mortality and worse functional
A decision analysis. Stroke 2003; 34: 1710–16. outcome after intracerebral hemorrhage. Neurocrit Care 2010;
161 Greenberg SM, Eng JA, Ning M, Smith EE, Rosand J. Hemorrhage 13: 67–74.
burden predicts recurrent intracerebral hemorrhage after lobar 176 Lee SH, Kim BJ, Bae HJ, et al. Effects of glucose level on early and
hemorrhage. Stroke 2004; 35: 1415–20. long-term mortality after intracerebral haemorrhage: the Acute
162 Commichau C, Scarmeas N, Mayer SA. Risk factors for fever in the Brain Bleeding Analysis Study. Diabetologia 2010; 53: 429–34.
neurologic intensive care unit. Neurology 2003; 60: 837–41. 177 Qureshi AI, Palesch YY, Martin R, et al; ATACH Investigators.
163 Schwarz S, Häfner K, Aschoff A, Schwab S. Incidence and Association of serum glucose concentrations during acute
prognostic significance of fever following intracerebral hemorrhage. hospitalization with hematoma expansion, perihematomal edema,
Neurology 2000; 54: 354–61. and three month outcome among patients with intracerebral
164 den Hertog HM, van der Worp HB, van Gemert HM, van Gijn J, hemorrhage. Neurocrit Care 2011 May 15 [Epub ahead of print].
Koudstaal PJ, Dippel DW. Effects of high-dose paracetamol on blood 178 Weir CJ, Murray GD, Dyker AG, Lees KR. Is hyperglycaemia an
pressure in acute stroke. Acta Neurol Scand 2011; published online independent predictor of poor outcome after acute stroke? Results
June 8. DOI:10.1111/j.1600-0404.2011.01529.x [Epub ahead of print]. of a long term follow up study. BMJ 1997; 314: 1303–06.
165 Hajat C, Hajat S, Sharma P. Effects of poststroke pyrexia on stroke 179 Gray CS, Hildreth AJ, Sandercock PA, et al, and the GIST Trialists
outcome: a meta-analysis of studies in patients. Stroke 2000; Collaboration. Glucose-potassium-insulin infusions in the
31: 410–14. management of post-stroke hyperglycaemia: the UK Glucose
166 Reith J, Jørgensen HS, Pedersen PM, et al. Body temperature in Insulin in Stroke Trial (GIST-UK). Lancet Neurol 2007; 6: 397–406.
acute stroke: relation to stroke severity, infarct size, mortality, and 180 Qureshi AI. Acute hypertensive response in patients with stroke:
outcome. Lancet 1996; 347: 422–25. pathophysiology and management. Circulation 2008; 118: 176–87.
167 Greer DM, Funk SE, Reaven NL, Ouzounelli M, Uman GC. Impact 181 Qureshi AI, Ezzeddine MA, Nasar A, et al. Prevalence of elevated
of fever on outcome in patients with stroke and neurologic injury: blood pressure in 563 704 adult patients with stroke presenting to
a comprehensive meta-analysis. Stroke 2008; 39: 3029–35. the ED in the United States. Am J Emerg Med 2007; 25: 32–38.
168 den Hertog HM, van der Worp HB, van Gemert HM, et al, and the 182 Willmot M, Leonardi-Bee J, Bath PM. High blood pressure in acute
PAIS Investigators. The Paracetamol (Acetaminophen) In Stroke stroke and subsequent outcome: a systematic review. Hypertension
(PAIS) trial: a multicentre, randomised, placebo-controlled, 2004; 43: 18–24.
phase III trial. Lancet Neurol 2009; 8: 434–40. 183 Zhang Y, Reilly KH, Tong W, et al. Blood pressure and clinical
169 Rincon F, Mayer SA. Clinical review: Critical care management of outcome among patients with acute stroke in Inner Mongolia,
spontaneous intracerebral hemorrhage. Crit Care 2008; 12: 237. China. J Hypertens 2008; 26: 1446–52.
170 Georgilis K, Plomaritoglou A, Dafni U, Bassiakos Y, Vemmos K. 184 Vemmos KN, Tsivgoulis G, Spengos K, et al. U-shaped relationship
Aetiology of fever in patients with acute stroke. J Intern Med 1999; between mortality and admission blood pressure in patients with
246: 203–09. acute stroke. J Intern Med 2004; 255: 257–65.
118 www.thelancet.com/neurology Vol 11 January 2012
You might also like
- CCT AsqDocument12 pagesCCT Asqlcando100% (1)
- AWC SDPWS2015 Commentary PrintableDocument52 pagesAWC SDPWS2015 Commentary PrintableTerry TriestNo ratings yet
- Rebranding Brief TemplateDocument8 pagesRebranding Brief TemplateRushiraj Patel100% (1)
- Benzon CaseDocument3 pagesBenzon Casejulieanne07100% (1)
- DSA NotesDocument87 pagesDSA NotesAtefrachew SeyfuNo ratings yet
- Anesth Analg 2010 Elliott 1419 27Document9 pagesAnesth Analg 2010 Elliott 1419 27Darrel Allan MandiasNo ratings yet
- Intracranialhemorrhage: J. Alfredo Caceres,, Joshua N. GoldsteinDocument24 pagesIntracranialhemorrhage: J. Alfredo Caceres,, Joshua N. GoldsteinReyhan AristoNo ratings yet
- Intracranialhemorrhage: J. Alfredo Caceres,, Joshua N. GoldsteinDocument24 pagesIntracranialhemorrhage: J. Alfredo Caceres,, Joshua N. GoldsteinLyaNo ratings yet
- Acv Hemorragico Tto 2014Document19 pagesAcv Hemorragico Tto 2014DIANA LIZETH NIÑO SAAVEDRANo ratings yet
- HIC Acute CNA 2016Document17 pagesHIC Acute CNA 2016Ellys Macías PeraltaNo ratings yet
- Kaplovitch 2020Document16 pagesKaplovitch 2020Verónica Rojas NavaNo ratings yet
- Intracerebral HemorrhageDocument39 pagesIntracerebral HemorrhageBush HsiehNo ratings yet
- Intracerebral Hemorrhage Medical TreatmentDocument3 pagesIntracerebral Hemorrhage Medical TreatmentDarrel Allan MandiasNo ratings yet
- Emergency Care Advances for Intracerebral HemorrhageDocument14 pagesEmergency Care Advances for Intracerebral Hemorrhagecoyotito961No ratings yet
- Chronic Thromboembolic Pulmonary HypertensionDocument17 pagesChronic Thromboembolic Pulmonary HypertensionsunhaolanNo ratings yet
- Hypertension in Hematologic Malignancies and Hematopoietic Cell Transplantation: An Emerging Issue With The Introduction of Novel TreatmentsDocument8 pagesHypertension in Hematologic Malignancies and Hematopoietic Cell Transplantation: An Emerging Issue With The Introduction of Novel TreatmentsGabryelNo ratings yet
- Hemorrhagic Transformation After Cerebral InfarctionDocument14 pagesHemorrhagic Transformation After Cerebral InfarctionAlyk Tumayan CalionNo ratings yet
- Konstantinou Et Al-2019-The Journal of Clinical HypertensionDocument9 pagesKonstantinou Et Al-2019-The Journal of Clinical HypertensionAbdurrahman SamarqandyNo ratings yet
- Pulmonary Embolism - European Heart Journal 2012Document12 pagesPulmonary Embolism - European Heart Journal 2012Andreas IoannouNo ratings yet
- s40560-017-0223-2Document10 pagess40560-017-0223-2ERICK KUMAR BAUTISTA GOMEZNo ratings yet
- Platelet Count Predicts Post-Endoscopy Bleeding Risk in ChildrenDocument4 pagesPlatelet Count Predicts Post-Endoscopy Bleeding Risk in ChildrenMasri YaniNo ratings yet
- Emergency Management of Intracerebral HemorrhageDocument7 pagesEmergency Management of Intracerebral HemorrhageHey AndyNo ratings yet
- Case StudyDocument10 pagesCase StudyAumkar Bhai LadNo ratings yet
- Larsen Et Al 2020 Study of Antithrombotic Treatment After Intracerebral Haemorrhage Protocol For A RandomisedDocument9 pagesLarsen Et Al 2020 Study of Antithrombotic Treatment After Intracerebral Haemorrhage Protocol For A RandomisedDanuNo ratings yet
- Managing Massive HemoptysisDocument12 pagesManaging Massive Hemoptysisdoc_next_doorNo ratings yet
- Standard Treatment Guidelines Interventional Radiology: Ministry of Health & Family Welfare Govt. of IndiaDocument75 pagesStandard Treatment Guidelines Interventional Radiology: Ministry of Health & Family Welfare Govt. of IndiaKaustubhNo ratings yet
- Research Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionDocument9 pagesResearch Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionmikeNo ratings yet
- Management of Spontaneous Intracerebral Hemorrhage: Stroke (H Diener, Section Editor)Document11 pagesManagement of Spontaneous Intracerebral Hemorrhage: Stroke (H Diener, Section Editor)Deby AnditaNo ratings yet
- Tromboembolismo Pulmonar Manejo PDFDocument7 pagesTromboembolismo Pulmonar Manejo PDFGeovannaHGNo ratings yet
- Cranio Review 2Document6 pagesCranio Review 2Achmad FitrahNo ratings yet
- Angio$Document2 pagesAngio$Muthu KumarNo ratings yet
- Deep Venous Thrombosis 2022. ANNALSDocument20 pagesDeep Venous Thrombosis 2022. ANNALSErnesto LainezNo ratings yet
- How I Treat Hyperleukocytosis in Acute Myeloid LeukemiaDocument7 pagesHow I Treat Hyperleukocytosis in Acute Myeloid LeukemiaMarcela PauletteNo ratings yet
- Management of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHDocument10 pagesManagement of Hemostatic Complications in Acute Leukemia: Guidance From The SSC of The ISTHCarlos Enrique Almonte MarínNo ratings yet
- Ying Li 2016Document8 pagesYing Li 2016Bogdan TrandafirNo ratings yet
- Critical Care and Emergency Medicine Neurology in StrokeDocument3 pagesCritical Care and Emergency Medicine Neurology in StrokeAnca GuțuNo ratings yet
- Eajm 51 2 186Document5 pagesEajm 51 2 186Javier CarreraNo ratings yet
- Piis1052305713004734 PDFDocument7 pagesPiis1052305713004734 PDFbellaNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITPDocument11 pagesIdiopathic Thrombocytopenic Purpura (ITPMelDred Cajes BolandoNo ratings yet
- Diagnostics 10 01046 v2Document20 pagesDiagnostics 10 01046 v2M Halis HermawanNo ratings yet
- Trends in Cardiovascular Medicine: Lauren Sinnenberg, Michael M. GivertzDocument9 pagesTrends in Cardiovascular Medicine: Lauren Sinnenberg, Michael M. GivertzJulio PorrasNo ratings yet
- Hipertrofia VD en HTADocument8 pagesHipertrofia VD en HTAgustavo reyesNo ratings yet
- 16Document8 pages16AlamgirNo ratings yet
- Lapkas Ilmu Penyakit Saraf Stroke HaemoragikdocxDocument4 pagesLapkas Ilmu Penyakit Saraf Stroke HaemoragikdocxAnonymous XO9RqHhOgiNo ratings yet
- Fonc 11 640999Document13 pagesFonc 11 640999desconocido 123 ambticonNo ratings yet
- Thromboembolic Complications in Chronic Inflammatory Bowel DiseaseDocument6 pagesThromboembolic Complications in Chronic Inflammatory Bowel DiseaseIJAR JOURNALNo ratings yet
- White-Coat Hypertension, As Defined by Ambulatory Blood Pressure Monitoring, and Subclinical Cardiac Organ Damage: A Meta-AnalysisDocument9 pagesWhite-Coat Hypertension, As Defined by Ambulatory Blood Pressure Monitoring, and Subclinical Cardiac Organ Damage: A Meta-AnalysisyuyunzilaNo ratings yet
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionDocument7 pagesMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesNo ratings yet
- Editor 'S Choice e Cerebral Hyperperfusion Syndrome After Carotid Artery Stenting: A Systematic Review and Meta-AnalysisDocument12 pagesEditor 'S Choice e Cerebral Hyperperfusion Syndrome After Carotid Artery Stenting: A Systematic Review and Meta-AnalysisanankastikNo ratings yet
- Hta (G4)Document9 pagesHta (G4)Juan LeonNo ratings yet
- Management of Cardiogenic Shock: Clinical UpdateDocument10 pagesManagement of Cardiogenic Shock: Clinical Updateaswad 0008No ratings yet
- Embolia Pulmonar SubmasivaDocument27 pagesEmbolia Pulmonar SubmasivaLuis Fernando Morales JuradoNo ratings yet
- tmp331B TMPDocument10 pagestmp331B TMPFrontiersNo ratings yet
- E2f7 PDFDocument7 pagesE2f7 PDFSujith KumarNo ratings yet
- Thrombolytic Therapy For Ischemic StrokeDocument7 pagesThrombolytic Therapy For Ischemic StrokechandradwtrNo ratings yet
- 2020 - Ribeiro - RNA Splicing Defects in HCM Implications For Diagnosis and TherapyDocument17 pages2020 - Ribeiro - RNA Splicing Defects in HCM Implications For Diagnosis and Therapymarta ribeiroNo ratings yet
- Fenger Eriksen2019Document8 pagesFenger Eriksen2019cynthia ventura bordaNo ratings yet
- The FASEB Journal - 2023 - Pathophysiology and targeted treatment of cholesterol crystal embolismDocument16 pagesThe FASEB Journal - 2023 - Pathophysiology and targeted treatment of cholesterol crystal embolismA. GilesNo ratings yet
- Ramirez Garzon Ibarra Consideraciones Perioperatorias en Pacientes Hipertensos RevChAn23Document7 pagesRamirez Garzon Ibarra Consideraciones Perioperatorias en Pacientes Hipertensos RevChAn23Fel MercNo ratings yet
- TEP Systemic Thrombolysis For Pulmonary Embolism Evidence, Patient Selection, and Protocols For ManagementDocument10 pagesTEP Systemic Thrombolysis For Pulmonary Embolism Evidence, Patient Selection, and Protocols For Managementbenitez1228No ratings yet
- UntitledDocument7 pagesUntitledYulian 53No ratings yet
- PneuDocument9 pagesPneutego_sulistyonoNo ratings yet
- English Progress Program: Nama: Nurul Hidayah NIM: 21117091Document12 pagesEnglish Progress Program: Nama: Nurul Hidayah NIM: 21117091nurul4hidayah-99No ratings yet
- EMU 2012 Massive TransfusionDocument8 pagesEMU 2012 Massive TransfusionjohnshenryNo ratings yet
- Secondary HypertensionFrom EverandSecondary HypertensionAlberto MorgantiNo ratings yet
- Tata Chemicals Yearly Reports 2019 20Document340 pagesTata Chemicals Yearly Reports 2019 20AkchikaNo ratings yet
- Comparing Time Series Models to Predict Future COVID-19 CasesDocument31 pagesComparing Time Series Models to Predict Future COVID-19 CasesManoj KumarNo ratings yet
- KDL 23S2000Document82 pagesKDL 23S2000Carlos SeguraNo ratings yet
- Ieee Research Papers On Software Testing PDFDocument5 pagesIeee Research Papers On Software Testing PDFfvgjcq6a100% (1)
- Gattu Madhuri's Resume for ECE GraduateDocument4 pagesGattu Madhuri's Resume for ECE Graduatedeepakk_alpineNo ratings yet
- The Human Resource Department of GIK InstituteDocument1 pageThe Human Resource Department of GIK InstitutexandercageNo ratings yet
- CORE Education Bags Rs. 120 Cr. Order From Gujarat Govt.Document2 pagesCORE Education Bags Rs. 120 Cr. Order From Gujarat Govt.Sanjeev MansotraNo ratings yet
- Abb Drives: User'S Manual Flashdrop Mfdt-01Document62 pagesAbb Drives: User'S Manual Flashdrop Mfdt-01Сергей СалтыковNo ratings yet
- ANDRITZ Company Presentation eDocument6 pagesANDRITZ Company Presentation eAnonymous OuY6oAMggxNo ratings yet
- Pig PDFDocument74 pagesPig PDFNasron NasirNo ratings yet
- Make a Battery Level Indicator using LM339 ICDocument13 pagesMake a Battery Level Indicator using LM339 ICnelson100% (1)
- NAC Case Study AnalysisDocument25 pagesNAC Case Study AnalysisSushma chhetriNo ratings yet
- Green Management: Nestlé's Approach To Green Management 1. Research and DevelopmentDocument6 pagesGreen Management: Nestlé's Approach To Green Management 1. Research and DevelopmentAbaidullah TanveerNo ratings yet
- Bar Exam 2016 Suggested Answers in Political LawDocument15 pagesBar Exam 2016 Suggested Answers in Political LawYlnne Cahlion KiwalanNo ratings yet
- OBHR Case StudyDocument8 pagesOBHR Case StudyYvonne TanNo ratings yet
- WitepsolDocument21 pagesWitepsolAnastasius HendrianNo ratings yet
- Erp and Mis Project - Thanks To PsoDocument31 pagesErp and Mis Project - Thanks To PsoAkbar Syed100% (1)
- Queries With AND and OR OperatorsDocument29 pagesQueries With AND and OR OperatorstrivaNo ratings yet
- Operation Roman Empire Indictment Part 1Document50 pagesOperation Roman Empire Indictment Part 1Southern California Public RadioNo ratings yet
- Planning For Network Deployment in Oracle Solaris 11.4: Part No: E60987Document30 pagesPlanning For Network Deployment in Oracle Solaris 11.4: Part No: E60987errr33No ratings yet
- PTAS-11 Stump - All About Learning CurvesDocument43 pagesPTAS-11 Stump - All About Learning CurvesinSowaeNo ratings yet
- Pyrometallurgical Refining of Copper in An Anode Furnace: January 2005Document13 pagesPyrometallurgical Refining of Copper in An Anode Furnace: January 2005maxi roaNo ratings yet
- Difference Between OS1 and OS2 Single Mode Fiber Cable - Fiber Optic Cabling SolutionsDocument2 pagesDifference Between OS1 and OS2 Single Mode Fiber Cable - Fiber Optic Cabling SolutionsDharma Teja TanetiNo ratings yet
- SDNY - Girl Scouts V Boy Scouts ComplaintDocument50 pagesSDNY - Girl Scouts V Boy Scouts Complaintjan.wolfe5356No ratings yet
- ITS America's 2009 Annual Meeting & Exposition: Preliminary ProgramDocument36 pagesITS America's 2009 Annual Meeting & Exposition: Preliminary ProgramITS AmericaNo ratings yet