You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Iap Ped IcuDocument375 pagesIap Ped IcuNguyen van ChienNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- qb19 - Media Notes - Am A-L PDFDocument171 pagesqb19 - Media Notes - Am A-L PDFHarry CramerNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Classification ASA y Perioperative VariablesDocument7 pagesClassification ASA y Perioperative VariablesEugenio Martinez HurtadoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- ANESTHESIOLOGY 2019 From A Third Year Medical Student's PerspectiveDocument10 pagesANESTHESIOLOGY 2019 From A Third Year Medical Student's PerspectiveSatyam PandeyNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- NURS 682 Care Coordination and Role of The Advanced Practice NurseDocument9 pagesNURS 682 Care Coordination and Role of The Advanced Practice NurseParya VNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Diretrizes de Dor Agitacao Delirium Imobilidade e Sono PADIS Guidelines Portuguese TranslationDocument58 pagesDiretrizes de Dor Agitacao Delirium Imobilidade e Sono PADIS Guidelines Portuguese TranslationGabriel LimaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Pts PTR Rev 4.1.21Document4 pagesPts PTR Rev 4.1.21M JainNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Administration Errors in SEADocument7 pagesAdministration Errors in SEAFrancis NgNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- How To Dominate The Ventilator: Spinning DialsDocument5 pagesHow To Dominate The Ventilator: Spinning DialsIgnacia Cid PintoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Lecture 4 Airway Devices pr2 - 090848Document75 pagesLecture 4 Airway Devices pr2 - 090848Abed AlawnehNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Anesth Analg 2019 129 6 1504-11Document8 pagesAnesth Analg 2019 129 6 1504-11Fernando SousaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Conscious Sedation PaediatricsDocument44 pagesConscious Sedation PaediatricsReeta TaxakNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- As ISO 7376.3-2002 Laryngoscopic Fittings Fibre-Illuminated Re-Usable Rigid LaryngoscopesDocument8 pagesAs ISO 7376.3-2002 Laryngoscopic Fittings Fibre-Illuminated Re-Usable Rigid LaryngoscopesSAI Global - APACNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Local AnaesthesiaDocument4 pagesLocal AnaesthesiaFaria Islam Juhi100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Drug Study On AnestheticsDocument9 pagesDrug Study On AnestheticsKalvinArtRazalanCelebradosNo ratings yet
- Surgery at AIC Kijabe Hospital in Rural Kenya: C G H DDocument32 pagesSurgery at AIC Kijabe Hospital in Rural Kenya: C G H DAR RafiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anesthesia - Anesthesiology, Surgery, Side Effects, Types, RiskDocument1 pageAnesthesia - Anesthesiology, Surgery, Side Effects, Types, RiskAbdussalam AboubakerNo ratings yet
- Clasificacion Asa 2019 PDFDocument2 pagesClasificacion Asa 2019 PDFMaria Alejandra Atencio100% (1)
- Presentation DetailsDocument2 pagesPresentation DetailsAnkit NagvekarNo ratings yet
- Recommended Reading List For EDAICDocument4 pagesRecommended Reading List For EDAICAna Belén Artero CastañoNo ratings yet
- TM 6Document13 pagesTM 6Tya DwiNo ratings yet
- Anaesthesia RCOphth GuidelinesDocument4 pagesAnaesthesia RCOphth GuidelinesDiana SmithNo ratings yet
- Anaesthesia HandoutDocument2 pagesAnaesthesia HandouttytrytrNo ratings yet
- Ma 661Document46 pagesMa 661Ale AaoNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Cpap - Ventilator - Respiratory - Suction - Nebulizer Product CatalogDocument92 pagesCpap - Ventilator - Respiratory - Suction - Nebulizer Product Catalogvirgini janetNo ratings yet
- Final Exam National Board of Examinations JUNE 2019 Anaesthesiology Paper-IiDocument2 pagesFinal Exam National Board of Examinations JUNE 2019 Anaesthesiology Paper-IiPrem KotiNo ratings yet
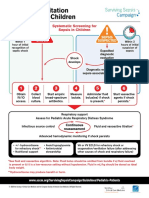
- PED Surviving Sepsis AlgorithmDocument2 pagesPED Surviving Sepsis AlgorithmDaniel Cruz de AbreuNo ratings yet
- F 360Document6 pagesF 360اسعد عبد الحميد50% (2)
- @anesthesia Books 2013 Rapid Review PDFDocument262 pages@anesthesia Books 2013 Rapid Review PDFLuminița Lumi100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Starmed Range: Providing A Choice of Interface For Your PatientsDocument6 pagesThe Starmed Range: Providing A Choice of Interface For Your PatientshelenaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)