You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Standard Operating Procedure (Sop) of - High Performance Liquid Chromatography System (HPLC)Document9 pagesStandard Operating Procedure (Sop) of - High Performance Liquid Chromatography System (HPLC)sandeep raiNo ratings yet
- IJMLR231710Document4 pagesIJMLR231710sandeep raiNo ratings yet
- IJMLR231709Document8 pagesIJMLR231709sandeep raiNo ratings yet
- Ijmlr231702 PDFDocument7 pagesIjmlr231702 PDFsandeep raiNo ratings yet
- IJMLR231705Document7 pagesIJMLR231705sandeep raiNo ratings yet
- IJMLR231703Document5 pagesIJMLR231703sandeep raiNo ratings yet
- Department of Pharmaceutical Analysis, V. V. Institute of Pharmaceutical Sciences, Gudlavalleru, A.P., IndiaDocument11 pagesDepartment of Pharmaceutical Analysis, V. V. Institute of Pharmaceutical Sciences, Gudlavalleru, A.P., Indiasandeep raiNo ratings yet
- Kidney Functions in Wister Rats Treated WTH Artesunate and AmodiaquineDocument5 pagesKidney Functions in Wister Rats Treated WTH Artesunate and Amodiaquinesandeep raiNo ratings yet
- IJMLR311809Document6 pagesIJMLR311809sandeep raiNo ratings yet
- IJMLR231707Document6 pagesIJMLR231707sandeep raiNo ratings yet
- IJMLR231704Document7 pagesIJMLR231704sandeep raiNo ratings yet
- IJMLR231701Document6 pagesIJMLR231701sandeep raiNo ratings yet
- Research Article: ISSN No. 2456-4400 Int J Med Lab Res 2018, 3 (1) : 39-45Document7 pagesResearch Article: ISSN No. 2456-4400 Int J Med Lab Res 2018, 3 (1) : 39-45sandeep raiNo ratings yet
- IJMLR311804Document6 pagesIJMLR311804sandeep raiNo ratings yet
- IJMLR311802Document9 pagesIJMLR311802sandeep raiNo ratings yet
- Study of Pre Analytical Errors in A Medium Sized Pathology LaboratoryDocument6 pagesStudy of Pre Analytical Errors in A Medium Sized Pathology Laboratorysandeep raiNo ratings yet
- Utility of Lamp Assay in Early Detection of Dengue Virus InfectionDocument6 pagesUtility of Lamp Assay in Early Detection of Dengue Virus Infectionsandeep raiNo ratings yet
- IJMLR311808Document3 pagesIJMLR311808sandeep raiNo ratings yet
- Parvovirus B19 Infection and Transient Aplastic Crisis Kaveh TariDocument7 pagesParvovirus B19 Infection and Transient Aplastic Crisis Kaveh Tarisandeep raiNo ratings yet
- IJMLR311801Document5 pagesIJMLR311801sandeep raiNo ratings yet
- IJMLR311803Document6 pagesIJMLR311803sandeep raiNo ratings yet
- IJMLR121601Document5 pagesIJMLR121601sandeep raiNo ratings yet
- IJMLR121603Document7 pagesIJMLR121603sandeep raiNo ratings yet
- Quality Determinants For Medical Histology Laboratory: (Ijmlr)Document11 pagesQuality Determinants For Medical Histology Laboratory: (Ijmlr)sandeep raiNo ratings yet
- Approaches in The Treatment of Diabetes Mellitus: Sahoo Et Al., Int J Med Lab Res, 1 (2) : 29-37Document9 pagesApproaches in The Treatment of Diabetes Mellitus: Sahoo Et Al., Int J Med Lab Res, 1 (2) : 29-37sandeep raiNo ratings yet
- IJMLR121602Document4 pagesIJMLR121602sandeep raiNo ratings yet
- Analysis of Phosphine With Different TechniquesDocument7 pagesAnalysis of Phosphine With Different Techniquessandeep raiNo ratings yet
- IJMLR211707Document7 pagesIJMLR211707sandeep raiNo ratings yet
- HPV: Infection, Prevention and Vaccination in India: Ritesh KumarDocument6 pagesHPV: Infection, Prevention and Vaccination in India: Ritesh Kumarsandeep raiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ang Kwento ni RosarioDocument2 pagesAng Kwento ni RosarioDarwin AndalNo ratings yet
- MSA in STIDocument36 pagesMSA in STISuhazeli Abdullah100% (2)
- MICROPARADocument8 pagesMICROPARAKloe Mari B.No ratings yet
- Auditing Hospital Associated InfectionsDocument59 pagesAuditing Hospital Associated Infectionstummalapalli venkateswara raoNo ratings yet
- Bds SyllabusDocument67 pagesBds Syllabusabdulbasitejaz100% (2)
- Battling Resistance To Antibiotics and PesticidesDocument399 pagesBattling Resistance To Antibiotics and PesticidesenglishwomanNo ratings yet
- 04 Shankar Rajasekaran - Design and Testing of Unidirectional Air Flow SystemsDocument38 pages04 Shankar Rajasekaran - Design and Testing of Unidirectional Air Flow SystemsVignesh BalajiNo ratings yet
- Checklist On Donning (Putting On) PPE: Personal Protective Equipment (PPE)Document5 pagesChecklist On Donning (Putting On) PPE: Personal Protective Equipment (PPE)Jan Oliver YaresNo ratings yet
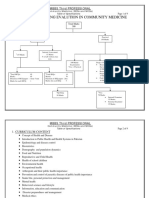
- Flow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalDocument9 pagesFlow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalusamaNo ratings yet
- Neuropathic Diabetic Foot Ulcers: Clinical PracticeDocument8 pagesNeuropathic Diabetic Foot Ulcers: Clinical PracticeAnisa SafutriNo ratings yet
- Immunostimulants enhance immunity through multiple pathwaysDocument7 pagesImmunostimulants enhance immunity through multiple pathwaysTanmay MehtaNo ratings yet
- Introduction To VirologyDocument8 pagesIntroduction To VirologyBeck ParkerNo ratings yet
- Vocabulary HealthDocument3 pagesVocabulary HealthmyassinedehbiNo ratings yet
- Relations of Protein, Zinc, Iron Intake, Infectious Diseases and H/A Z-Score in Children Aged 24-59 MonthsDocument24 pagesRelations of Protein, Zinc, Iron Intake, Infectious Diseases and H/A Z-Score in Children Aged 24-59 MonthsdaniNo ratings yet
- Dialysis Wall Boxes and Drains - Dialysis Safety - CDCDocument2 pagesDialysis Wall Boxes and Drains - Dialysis Safety - CDCNur Aqilah IsmailNo ratings yet
- Healthy Ways Newsletter 9-4 by Bruce FifeDocument23 pagesHealthy Ways Newsletter 9-4 by Bruce FifeAmanda Velasquez100% (1)
- Sputum AnalysisDocument12 pagesSputum AnalysisAdriana GarciaNo ratings yet
- Class 8th Assignment 2024Document42 pagesClass 8th Assignment 2024anooshaaaa.23No ratings yet
- WHO On Tuberculosis: Operational HandbookDocument140 pagesWHO On Tuberculosis: Operational HandbookYenny BelindaNo ratings yet
- Three-Combination Probiotics Therapy in Children With Salmonella and Rotavirus GastroenteritisDocument6 pagesThree-Combination Probiotics Therapy in Children With Salmonella and Rotavirus Gastroenteritisnadin nNo ratings yet
- Puerperal Infection of The Genital TractDocument11 pagesPuerperal Infection of The Genital TractNatalia Vasquez MedicoNo ratings yet
- "Ni-Raspa Ako Dahil Nalalag Yung Baby Ko." As Verbalized byDocument1 page"Ni-Raspa Ako Dahil Nalalag Yung Baby Ko." As Verbalized byMary AgorillaNo ratings yet
- Label Pediapred Ngu N FDADocument13 pagesLabel Pediapred Ngu N FDAHuyền LêNo ratings yet
- Research, A Peer-Reviewed Medical Journal Published by Elsevier. Please SeeDocument87 pagesResearch, A Peer-Reviewed Medical Journal Published by Elsevier. Please SeeFilipos ConstantinNo ratings yet
- The Use of Mathematical Models in Epidemiological Study of Infectious Diseases and in The Design of Mass Immunization ProgrammesDocument21 pagesThe Use of Mathematical Models in Epidemiological Study of Infectious Diseases and in The Design of Mass Immunization ProgrammesAhmed EshebliNo ratings yet
- Contamination Control in Healthcare Product Manufacturing Volume 5 - ContenidoDocument11 pagesContamination Control in Healthcare Product Manufacturing Volume 5 - Contenidocargscrib100% (1)
- Handouts CD Prof. RojasDocument6 pagesHandouts CD Prof. RojasChallen CulturaNo ratings yet
- Different Field of Medical Specialization: July 2020Document3 pagesDifferent Field of Medical Specialization: July 2020Ari :3No ratings yet
- Syllabus 112Document9 pagesSyllabus 112Hassen Zabala100% (2)
- CDC guidelines for treating syphilisDocument27 pagesCDC guidelines for treating syphilisGabrielaGushikenNo ratings yet