You might also like
- Lecture notes on human respiratory system physiologyDocument33 pagesLecture notes on human respiratory system physiologyMiles HuiNo ratings yet
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsFrom EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNo ratings yet
- Copd and Equal Pressure PointDocument3 pagesCopd and Equal Pressure Pointleh.mo9315No ratings yet
- Should We Use Driving Pressure To Set Tidal Volume? PDFDocument7 pagesShould We Use Driving Pressure To Set Tidal Volume? PDFYaxkin NikNo ratings yet
- Mechanical Ventilation Dyssynchrony Types and ManagementDocument17 pagesMechanical Ventilation Dyssynchrony Types and ManagementjuanNo ratings yet
- Ventilator GraphicsDocument38 pagesVentilator GraphicsShaliniNo ratings yet
- Flow LoopDocument6 pagesFlow LoopfarexNo ratings yet
- Lung Sounds: An Assessment of The Patient in Respiratory DistressDocument40 pagesLung Sounds: An Assessment of The Patient in Respiratory DistressJoseph Rodney de LeonNo ratings yet
- Ecmo and SepsisDocument37 pagesEcmo and SepsisMarckus BrodyNo ratings yet
- NEJM 2014 Fundamentals of Lung AuscultationDocument7 pagesNEJM 2014 Fundamentals of Lung AuscultationFelipe CeaNo ratings yet
- Clinical ECG RoundsDocument2 pagesClinical ECG RoundsKai Siang ChanNo ratings yet
- Basics of Waveform Interpretation: RET 2284 Principles of Mechanical VentilationDocument66 pagesBasics of Waveform Interpretation: RET 2284 Principles of Mechanical VentilationNanda MinndinNo ratings yet
- Mechanical Ventilation Formulas and Norms Flashcards - QuizletDocument8 pagesMechanical Ventilation Formulas and Norms Flashcards - QuizletAnonymous mNQq7ojNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Refractory Septic ShockDocument5 pagesRefractory Septic ShockBrian Antonio Veramatos LopezNo ratings yet
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- Unstable Angina, STEMI, NSTEMI Diagnosis and ManagementDocument21 pagesUnstable Angina, STEMI, NSTEMI Diagnosis and ManagementNabil Mosharraf Hossain100% (2)
- OutputDocument12 pagesOutputzenishzalamNo ratings yet
- ICU Ventilator Dyssynchrony DiagnosisDocument12 pagesICU Ventilator Dyssynchrony DiagnosisBrenda Serrano LaraNo ratings yet
- Ventilator WaveformsDocument37 pagesVentilator Waveformsfifa_0304535No ratings yet
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument10 pagesVasoactive Agents For Adult Septic Shock: An Update and ReviewntnquynhproNo ratings yet
- Ventilator Grafik WeaponDocument6 pagesVentilator Grafik WeaponiqbalNo ratings yet
- Fluid Resuscitation - Dita AditianingsihDocument48 pagesFluid Resuscitation - Dita AditianingsihGalih Wicaksono100% (1)
- Mechanical Ventilation AulaDocument47 pagesMechanical Ventilation Aulaapi-3820606100% (1)
- Simple Office SpirometryDocument42 pagesSimple Office SpirometryRoberto Merza III100% (4)
- Respiratory and Renal ReviewDocument39 pagesRespiratory and Renal ReviewTony PadNo ratings yet
- PEEP (Positive-End Expiratory Pressure)Document5 pagesPEEP (Positive-End Expiratory Pressure)Valcrist BalderNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- Overview of Respiratory Failure & Mechanical VentilationDocument89 pagesOverview of Respiratory Failure & Mechanical VentilationsheharyarNo ratings yet
- How To Take A Set of Arterial Blood Gases (Abgs) : Think Lemon Juice in A Salted Paper Cut ..It Does Smart A Little!Document48 pagesHow To Take A Set of Arterial Blood Gases (Abgs) : Think Lemon Juice in A Salted Paper Cut ..It Does Smart A Little!shiv dattaNo ratings yet
- Cardiovascular Pathology 1:: Blood VesselsDocument48 pagesCardiovascular Pathology 1:: Blood VesselsRaiver CadenNo ratings yet
- Mechanical Ventilation GraphicsDocument144 pagesMechanical Ventilation GraphicsSaddamNo ratings yet
- Pulmonary Physiology NotesDocument18 pagesPulmonary Physiology Noteslezibells100% (2)
- Asthma and Rhinitis During PregnancyDocument175 pagesAsthma and Rhinitis During PregnancyAndika Wima PratamaNo ratings yet
- Sepsis WhoDocument36 pagesSepsis WholcycrlnNo ratings yet
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Idiopathic Pulmonary Fibrosis: Interstitial Lung DiseaseDocument5 pagesIdiopathic Pulmonary Fibrosis: Interstitial Lung DiseaseAmjaSaudNo ratings yet
- Pleural Disease LIGTHDocument0 pagesPleural Disease LIGTHKaisun TeoNo ratings yet
- Pulsus Paradoxus - Wikip PDFDocument4 pagesPulsus Paradoxus - Wikip PDFAniket MittalNo ratings yet
- Chest X-RayDocument101 pagesChest X-RayYuke04No ratings yet
- How Bloodis Propelled Throughthe Hum An Ci Rcula To Ry Sy StemDocument5 pagesHow Bloodis Propelled Throughthe Hum An Ci Rcula To Ry Sy Stemridwan100% (1)
- Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6e-17-31Document15 pagesPilbeam's Mechanical Ventilation Physiological and Clinical Applications 6e-17-31Lesly Peinado TorresNo ratings yet
- Use of Vasopressors and Inotropes - UpToDateDocument18 pagesUse of Vasopressors and Inotropes - UpToDateAlbertoMarteNo ratings yet
- Blue Protocol. Lung Ultrasound in The Critically IllDocument12 pagesBlue Protocol. Lung Ultrasound in The Critically IllRomina Alfonsina Decap CarrascoNo ratings yet
- The Treatment of Sepsis:: Early Goal Directed Therapy and BeyondDocument86 pagesThe Treatment of Sepsis:: Early Goal Directed Therapy and BeyondAndreas OctavianoNo ratings yet
- Pulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesDocument5 pagesPulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesIJAR JOURNALNo ratings yet
- Difficult Weaning From Cardiopulmonary Bypass Final Edit LiaDocument41 pagesDifficult Weaning From Cardiopulmonary Bypass Final Edit LiaYuri SadewoNo ratings yet
- Transposition of The Great VesselDocument30 pagesTransposition of The Great VesseljustinahorroNo ratings yet
- Atrial Systole: The End of DiastoleDocument9 pagesAtrial Systole: The End of DiastoleSophia MahboobNo ratings yet
- Pericardial EffusionDocument3 pagesPericardial EffusionNita Hurek100% (1)
- Waveform Questions /critical Care Board ReviewDocument14 pagesWaveform Questions /critical Care Board ReviewAzmachamberAzmacareNo ratings yet
- Mechanical VentilationDocument25 pagesMechanical VentilationmochkurniawanNo ratings yet
- Basics of Ventilatory SupportDocument43 pagesBasics of Ventilatory SupportAdhithya BhatNo ratings yet
- Ventricular Assist DeviceDocument12 pagesVentricular Assist DevicesamadonyNo ratings yet
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- 5.10 Cardiac AuscultationDocument47 pages5.10 Cardiac AuscultationDenisseRangelNo ratings yet
- The How-To of BiVent (APRV) Ventilation SettingsDocument63 pagesThe How-To of BiVent (APRV) Ventilation SettingsFarook BaigNo ratings yet
- Bio Rev CardsDocument21 pagesBio Rev CardsTamannaBhatiaNo ratings yet
- Updated: Dec 07, 2016 Author: Justina Gamache, MD Chief Editor: Guy W Soo Hoo, MD, MPHDocument42 pagesUpdated: Dec 07, 2016 Author: Justina Gamache, MD Chief Editor: Guy W Soo Hoo, MD, MPHgita suci arianiNo ratings yet
- GOLD Spirometry 2010Document59 pagesGOLD Spirometry 2010Ck Kma100% (1)
- H&PDocument3 pagesH&PCarlos Eduardo LinaresNo ratings yet
- Diffdx - 4X6 Cards - Post On VC2000 PDFDocument69 pagesDiffdx - 4X6 Cards - Post On VC2000 PDFCarlos Eduardo LinaresNo ratings yet
- Diffdx - 4X6 Cards - Post On VC2000 PDFDocument69 pagesDiffdx - 4X6 Cards - Post On VC2000 PDFCarlos Eduardo LinaresNo ratings yet
- Genes Molecules Cells Course ObjectivesDocument31 pagesGenes Molecules Cells Course ObjectivesCarlos Eduardo LinaresNo ratings yet
- Maize PosterDocument2 pagesMaize PosterCarlos Eduardo LinaresNo ratings yet
- Admission Note CL WEEK 3Document3 pagesAdmission Note CL WEEK 3Carlos Eduardo LinaresNo ratings yet
- Essay 2 CasesDocument8 pagesEssay 2 CasesCarlos Eduardo LinaresNo ratings yet
- Acid-Base Lecture NotesDocument10 pagesAcid-Base Lecture NotesCarlos Eduardo LinaresNo ratings yet
- Just Getting The Main RX Names Down : Antidepressants Mood StabilizersDocument1 pageJust Getting The Main RX Names Down : Antidepressants Mood StabilizersCarlos Eduardo LinaresNo ratings yet
- Essay 5 - OB GYN - Carlos LinaresDocument2 pagesEssay 5 - OB GYN - Carlos LinaresCarlos Eduardo LinaresNo ratings yet
- Exam 1 KeyDocument10 pagesExam 1 KeyCarlos Eduardo LinaresNo ratings yet
- CAHSEE Algebra 1 Student Text - UC Davis - August 2008Document137 pagesCAHSEE Algebra 1 Student Text - UC Davis - August 2008Dennis Ashendorf100% (1)
- L2 Water+Molecular+Interactions+Acid-Base-v+ 2Document24 pagesL2 Water+Molecular+Interactions+Acid-Base-v+ 2Carlos Eduardo LinaresNo ratings yet
- Take Home Message From Lecture 5Document33 pagesTake Home Message From Lecture 5Carlos Eduardo LinaresNo ratings yet
- 03 04 Skeletal Muscle HandoutDocument10 pages03 04 Skeletal Muscle HandoutCarlos Eduardo LinaresNo ratings yet
- CH 08Document17 pagesCH 08Carlos Eduardo LinaresNo ratings yet
- L4 Amino+Acids-v+ 2Document30 pagesL4 Amino+Acids-v+ 2Carlos Eduardo LinaresNo ratings yet
- L3 Nucleic+Acids-v+ 2Document23 pagesL3 Nucleic+Acids-v+ 2Carlos Eduardo LinaresNo ratings yet
- L1 Biological+Organization-v+ 2Document24 pagesL1 Biological+Organization-v+ 2Carlos Eduardo LinaresNo ratings yet
- L1 Biological+Organization-v+ 2Document24 pagesL1 Biological+Organization-v+ 2Carlos Eduardo LinaresNo ratings yet
- Laporan Kasus BronkopneumoniaDocument30 pagesLaporan Kasus BronkopneumoniaShifa Ali JannatinNo ratings yet
- PEDIDocument280 pagesPEDIMiraf MesfinNo ratings yet
- Pleural Effusion: PathophysiologyDocument6 pagesPleural Effusion: PathophysiologyNyamburaNo ratings yet
- COPD X Australian Guidelines For The Diagnosis and Management of Chronic Obstructive Pulmonary Disease - 2022 Update (MJA 2022)Document9 pagesCOPD X Australian Guidelines For The Diagnosis and Management of Chronic Obstructive Pulmonary Disease - 2022 Update (MJA 2022)Chih-I LeeNo ratings yet
- RC Infant Flow LP NCPAP System Workbook UG enDocument60 pagesRC Infant Flow LP NCPAP System Workbook UG enWandi PrasadhaNo ratings yet
- Drug-Assisted Intubation Guide for Emergency Airway ManagementDocument1 pageDrug-Assisted Intubation Guide for Emergency Airway ManagementMEKSELINA KALENDERNo ratings yet
- Bedside Teaching On Mechanical Ventilation: Submitted ToDocument8 pagesBedside Teaching On Mechanical Ventilation: Submitted ToManisha Shakya50% (2)
- Greek BTSDocument51 pagesGreek BTSIrene Chrysovalanto ThemistocleousNo ratings yet
- Pulmonary Function TestsDocument2 pagesPulmonary Function TestsNishanth SampathNo ratings yet
- Acute Bronchitis Chronic Bronchitis: PathophysiologyDocument2 pagesAcute Bronchitis Chronic Bronchitis: PathophysiologyHarimunsyi Anugerah PratamaNo ratings yet
- Internal MedicineDocument146 pagesInternal MedicineSh. RamNo ratings yet
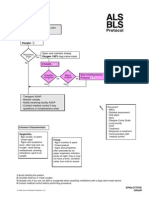
- Epiglottitis Croup ALS BLSDocument1 pageEpiglottitis Croup ALS BLStamara4668No ratings yet
- Shaker Deluxe Multi-Lingual ManualDocument4 pagesShaker Deluxe Multi-Lingual ManualcsavassNo ratings yet
- ARDSDocument57 pagesARDSnesjohnvNo ratings yet
- MEDION NOCAARC v310Document9 pagesMEDION NOCAARC v310Jinesh SanghviNo ratings yet
- Group 2a Presents on AsthmaDocument33 pagesGroup 2a Presents on AsthmaDalitso nkhomaNo ratings yet
- COPD Exacerbation TreatmentDocument7 pagesCOPD Exacerbation TreatmentAiman Arifin100% (1)
- Chronic BronchitisDocument19 pagesChronic BronchitisNurdina Afini100% (1)
- Pulmonary Function Test Results Visit Date 12/4/2018: FVC Fev1 FEV1%Document2 pagesPulmonary Function Test Results Visit Date 12/4/2018: FVC Fev1 FEV1%Shofiyyah ZahraNo ratings yet
- COPD Management with HFNCDocument58 pagesCOPD Management with HFNCpaionenseNo ratings yet
- Cairo: Pilbeam's Mechanical Ventilation, 6th EditionDocument6 pagesCairo: Pilbeam's Mechanical Ventilation, 6th Editionفاتن المطيريNo ratings yet
- How Ventilators Deliver BreathsDocument51 pagesHow Ventilators Deliver BreathsArnaldo SantizoNo ratings yet
- HematothoraxDocument15 pagesHematothoraxmail junkNo ratings yet
- Assessing and Managing Wheezing in Preschool ChildrenDocument8 pagesAssessing and Managing Wheezing in Preschool ChildrenEndy Widya PutrantoNo ratings yet
- COPD Pathophysiology, Assessment and Diagnosis GuideDocument20 pagesCOPD Pathophysiology, Assessment and Diagnosis GuideTony LeeNo ratings yet
- Emphysema 1Document7 pagesEmphysema 1ironNo ratings yet
- Chest and LungsDocument49 pagesChest and LungsChala KeneNo ratings yet
- Congenital Lobar EmphysemaDocument25 pagesCongenital Lobar Emphysemasheme1711No ratings yet
- DEZIDA - ARDS&CtraumaDocument3 pagesDEZIDA - ARDS&CtraumaCezanne CruzNo ratings yet
- RespirationDocument10 pagesRespirationADWAIT LALUNo ratings yet