You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 51 Phil JPub Admin 33Document19 pages51 Phil JPub Admin 33Jeff Cruz GregorioNo ratings yet
- Cheikh Anta Diop - Civilization or Barbarism. An Authentic AnthropologyDocument445 pagesCheikh Anta Diop - Civilization or Barbarism. An Authentic Anthropologywandersonn100% (5)
- The 2015-2020 Worldwide Digital English Language Learning MarketDocument27 pagesThe 2015-2020 Worldwide Digital English Language Learning MarketJesús LacónNo ratings yet
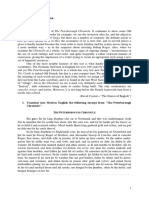
- Seminar 2 Middle English - Morphology - Peterborough-1Document2 pagesSeminar 2 Middle English - Morphology - Peterborough-1Isabela SincuNo ratings yet
- EU-Asia relations insightsDocument3 pagesEU-Asia relations insightsKatreddi Chandu Sai50% (4)
- Celebrating Freedom: APS Bolarum Marks Azadi Ka Amrit MahotsavDocument17 pagesCelebrating Freedom: APS Bolarum Marks Azadi Ka Amrit MahotsavGrey KoalaNo ratings yet
- Domestic Dimension of Public DiplomacyDocument12 pagesDomestic Dimension of Public DiplomacyJanno MoliaNo ratings yet
- 1989Document382 pages1989József GátasNo ratings yet
- Postal BallotDocument31 pagesPostal Ballotmukesh kumawatNo ratings yet
- Spark of Life - Erich Maria RemarqueDocument3 pagesSpark of Life - Erich Maria RemarqueYêu Văn HọcNo ratings yet
- English 4Q1 WK 7Document3 pagesEnglish 4Q1 WK 7Chinkay Clare CuenzNo ratings yet
- Ionesco's Rhinoceros - Analysis of Conformity and FascismDocument4 pagesIonesco's Rhinoceros - Analysis of Conformity and Fascismrupal arora100% (4)
- Lesson 4: The Contemporary Global GovernanceDocument5 pagesLesson 4: The Contemporary Global GovernanceMARK 2020No ratings yet
- Ap Gov ProjectDocument5 pagesAp Gov Projectapi-239946062No ratings yet
- Lesson 2.2Document8 pagesLesson 2.2Justmin CincoNo ratings yet
- Russia Ukraine and State Survival Through NeutraliDocument24 pagesRussia Ukraine and State Survival Through NeutraliCaesarGBNo ratings yet
- Utopia Bylaws 2019 2020Document15 pagesUtopia Bylaws 2019 2020Lawrence Gerald Lozada BerayNo ratings yet
- Gladys SourcesDocument3 pagesGladys Sourcesapi-510720727No ratings yet
- Thriller Survey Analysis: by Sasha and ShaniDocument8 pagesThriller Survey Analysis: by Sasha and Shanipinkbaby9No ratings yet
- The Letterman - (Available From 1st December)Document2 pagesThe Letterman - (Available From 1st December)Umoffia VictoriaNo ratings yet
- Maoz and Russett, Normative and Structural Causes of Democratic PeaceDocument16 pagesMaoz and Russett, Normative and Structural Causes of Democratic PeaceDebanjan BanerjeeNo ratings yet
- What Should I Know For Module 6?: 6.00: 19th Century Changes-IntroductionDocument17 pagesWhat Should I Know For Module 6?: 6.00: 19th Century Changes-IntroductiongoldenheartsNo ratings yet
- FBI Request for DNC, DCCC Hack DataDocument7 pagesFBI Request for DNC, DCCC Hack DataJay EllNo ratings yet
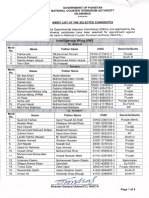
- Merit List of Selected CandidateDocument5 pagesMerit List of Selected CandidateAli Sher0% (1)
- LeaP UCSP Q4 Weeks 3 To 5 (JGF)Document7 pagesLeaP UCSP Q4 Weeks 3 To 5 (JGF)Jay FabellonNo ratings yet
- Nicknames: Famous Personalities of IndiaDocument22 pagesNicknames: Famous Personalities of IndiaRanaNo ratings yet
- Arthur Miller, An American Playwright: Death of A SalesmanDocument17 pagesArthur Miller, An American Playwright: Death of A SalesmanSophia McNamarah100% (1)
- A Rod PR LiderCon2021Document2 pagesA Rod PR LiderCon2021FluenceMediaNo ratings yet
- Hospital List As of FebDocument5 pagesHospital List As of FebRoy GonzaNo ratings yet
- 2768827Document16 pages2768827Muhammad Dian Saputra TaherNo ratings yet