You might also like
- Oral Ulcer Diseases DDDocument7 pagesOral Ulcer Diseases DDAmbar ZenNo ratings yet
- 1 s2.0 S2667147622000243 MainDocument4 pages1 s2.0 S2667147622000243 MainSoumya AnandanNo ratings yet
- Malignant Vs Traumatic Tongue Ulcer A Clinical AppDocument6 pagesMalignant Vs Traumatic Tongue Ulcer A Clinical Appvivi hutabaratNo ratings yet
- Condyloma Acuminatum: Some Aspects: Arūnas Rimkevičius, Alina Pūrienė, Mindaugas GaigalasDocument4 pagesCondyloma Acuminatum: Some Aspects: Arūnas Rimkevičius, Alina Pūrienė, Mindaugas GaigalasfaizawidiNo ratings yet
- Question:Discuss Various Malignancies of The Oral Region AnswersDocument6 pagesQuestion:Discuss Various Malignancies of The Oral Region AnswersMahdaba sheikh MohamudNo ratings yet
- Enfermedades InmunologicasDocument14 pagesEnfermedades InmunologicasKarina OjedaNo ratings yet
- Oral Leishmaniasis Report of Two Cases 2020Document5 pagesOral Leishmaniasis Report of Two Cases 2020MARIE SELENE RAMIREZ REVOLLARNo ratings yet
- Oral Findings in Secondary Syphilis: Zela Puteri Nurbani 1506668694Document15 pagesOral Findings in Secondary Syphilis: Zela Puteri Nurbani 1506668694adnanfananiNo ratings yet
- Exclusive Primary Lesion of Oral Leishmaniasis 2016Document5 pagesExclusive Primary Lesion of Oral Leishmaniasis 2016MARIE SELENE RAMIREZ REVOLLARNo ratings yet
- Journal 2.Document5 pagesJournal 2.Dha Dina SevofrationNo ratings yet
- Oropharyngeal Candidosis in The Older PatientDocument8 pagesOropharyngeal Candidosis in The Older Patientnugraheni.riniNo ratings yet
- PV 1Document4 pagesPV 1Aing ScribdNo ratings yet
- Jurnal MCP2Document4 pagesJurnal MCP2RENITA USWATUN HASANAH 1No ratings yet
- DX Dif Midline Destructive Disease 2014Document7 pagesDX Dif Midline Destructive Disease 2014MARIE SELENE RAMIREZ REVOLLARNo ratings yet
- International Journal of Infectious Diseases: Medical ImageryDocument3 pagesInternational Journal of Infectious Diseases: Medical Imageryfaty basalamahNo ratings yet
- Median Rhomboid Glossitis With Palatal 'Kissing Lesion'-A Case ReportDocument4 pagesMedian Rhomboid Glossitis With Palatal 'Kissing Lesion'-A Case ReportAninda Wulan PradaniNo ratings yet
- Articulo CientíficoDocument11 pagesArticulo CientíficoCarolina SalazarNo ratings yet
- PemfigusDocument5 pagesPemfigusSherlyNo ratings yet
- Median Rhomboid Glossitis in A Patient Undergoing Orthodontic TreatmentDocument4 pagesMedian Rhomboid Glossitis in A Patient Undergoing Orthodontic Treatmentandreia ichimNo ratings yet
- Oral Candidiasis An Overview and Case ReportDocument7 pagesOral Candidiasis An Overview and Case ReportPutri NingrumNo ratings yet
- 10.1515@sjdv 2016 0005Document6 pages10.1515@sjdv 2016 0005Gaby D'LuneNo ratings yet
- Oral Pemphigus Vulgaris: Corresponding Author: K Subadra, Ksubadra@sriramachandra - Edu.inDocument12 pagesOral Pemphigus Vulgaris: Corresponding Author: K Subadra, Ksubadra@sriramachandra - Edu.inDiva AzariaNo ratings yet
- Oral Submucous Fibrosis With Angular Cheilitis - A Case Scenario With Present Concepts On Aetiology and ManagementDocument6 pagesOral Submucous Fibrosis With Angular Cheilitis - A Case Scenario With Present Concepts On Aetiology and ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Case Report: Primary Malignant Melanoma of Maxilla: Report of A Case With DiscussionDocument5 pagesCase Report: Primary Malignant Melanoma of Maxilla: Report of A Case With DiscussionGina Kristina NanginNo ratings yet
- Papilloma Skuamosa: Laporan Kasus Dan Tinjauan PustakaDocument4 pagesPapilloma Skuamosa: Laporan Kasus Dan Tinjauan PustakarizkyayuarristaNo ratings yet
- Cavernous Hemangioma in The Floor of Oral Cavity Masquerading As A RanulaDocument5 pagesCavernous Hemangioma in The Floor of Oral Cavity Masquerading As A Ranula017Faradila Nayottama PutriNo ratings yet
- SCMS V34i4 White Lesions in The Oral CavityDocument10 pagesSCMS V34i4 White Lesions in The Oral CavityTasneem Hussiny AbdallahNo ratings yet
- A Large Oral Melanoma - A Case ReportDocument5 pagesA Large Oral Melanoma - A Case Reportfitri handayaniNo ratings yet
- Oral Squamous Cell Carcinoma Clinical Aspects: March 2012Document27 pagesOral Squamous Cell Carcinoma Clinical Aspects: March 2012Anh TranNo ratings yet
- Pemfigus VulgarisDocument5 pagesPemfigus VulgarisAgus LarobuNo ratings yet
- HPV InfectionDocument6 pagesHPV Infectionsrikantnairsemail8038No ratings yet
- Case Series Primary Oral TBDocument7 pagesCase Series Primary Oral TBAnggy Natya ListyaningrumNo ratings yet
- CR 4Document4 pagesCR 4Fitrah AndiNo ratings yet
- Extraoral and Intraoral Exam: Dentalelle TutoringDocument69 pagesExtraoral and Intraoral Exam: Dentalelle TutoringEviNo ratings yet
- Pleomorphic AdenomaDocument4 pagesPleomorphic AdenomaRobins DhakalNo ratings yet
- Rhadomyoma Mouth Floor OOOE 2010Document5 pagesRhadomyoma Mouth Floor OOOE 2010DrPrabhat Kumar TiwariNo ratings yet
- Long-Standing Oral Ulcers: Proposal For A New S-C-D Classification System'Document14 pagesLong-Standing Oral Ulcers: Proposal For A New S-C-D Classification System'Tegar Subeqi MochammadNo ratings yet
- 1 - Lesi Pigmentasi - Mifthaqul Istikhomah (40620124) KelompokDocument5 pages1 - Lesi Pigmentasi - Mifthaqul Istikhomah (40620124) KelompokAnggun PratiwiNo ratings yet
- TB UlcerDocument4 pagesTB UlcerKelvin BulainNo ratings yet
- Patología OralDocument11 pagesPatología OralLula Bá RdNo ratings yet
- NigerJClinPract21121674-5994143 163901Document4 pagesNigerJClinPract21121674-5994143 163901Adriana CardeñaNo ratings yet
- Oral Cancer: Nader A. Al-AizariDocument51 pagesOral Cancer: Nader A. Al-AizariNader AlaizariNo ratings yet
- Kanker MulutDocument2 pagesKanker MulutHamba AllahNo ratings yet
- Atypical TuberculosisDocument3 pagesAtypical TuberculosisWilda Khairani DalimuntheNo ratings yet
- Oral Cancer MADE EASYDocument19 pagesOral Cancer MADE EASYMohammedNo ratings yet
- MainDocument4 pagesMainMardhiatiNo ratings yet
- Oral Rhabdomyosarcoma A Case Report 2161 0681 3 161Document4 pagesOral Rhabdomyosarcoma A Case Report 2161 0681 3 161Nabila RizkikaNo ratings yet
- Oral Pathology in Paediatric Patients-Mini-Systematic ReviewDocument7 pagesOral Pathology in Paediatric Patients-Mini-Systematic ReviewYuganya SriNo ratings yet
- Oral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)Document14 pagesOral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)JohnNo ratings yet
- Herpes Zoster Infection of Maxillary and Mandibular BranchpoDocument4 pagesHerpes Zoster Infection of Maxillary and Mandibular BranchpovikriNo ratings yet
- Case Report: Oral Malignant Melanoma: A Rare Case With Unusual Clinical PresentationDocument5 pagesCase Report: Oral Malignant Melanoma: A Rare Case With Unusual Clinical PresentationA A Ngurah Wisnu Adiputra CNo ratings yet
- Mucosal Leishmaniasis With Primary Oral Involvement 2014Document9 pagesMucosal Leishmaniasis With Primary Oral Involvement 2014MARIE SELENE RAMIREZ REVOLLARNo ratings yet
- 1-Malignant Melanoma of The Oral Cavity A ReviewDocument3 pages1-Malignant Melanoma of The Oral Cavity A ReviewPaomo Zhixia EarlyNo ratings yet
- Common Oral Lesions: by Joseph Knight, PA-CDocument7 pagesCommon Oral Lesions: by Joseph Knight, PA-CAnonymous k8rDEsJsU1No ratings yet
- Oral Warts.: DR Nwachukwu N. CDocument19 pagesOral Warts.: DR Nwachukwu N. Cenwachukwu_1No ratings yet
- Verruca Vulgaris in A Non-Immunocompromised Patient: Case ReportDocument4 pagesVerruca Vulgaris in A Non-Immunocompromised Patient: Case ReportBryan Eliezer SitumorangNo ratings yet
- Periodontal Root Coverage: An Evidence-Based Guide to Prognosis and TreatmentFrom EverandPeriodontal Root Coverage: An Evidence-Based Guide to Prognosis and TreatmentNo ratings yet
- Melanocytic Lesions: A Case Based ApproachFrom EverandMelanocytic Lesions: A Case Based ApproachMai P. HoangNo ratings yet
- TaninDocument9 pagesTaninMuthia HannisaNo ratings yet
- Tanin PDFDocument9 pagesTanin PDFMuthia HannisaNo ratings yet
- The Effect of Extract Betel Leaf waterNEWRNGDocument1 pageThe Effect of Extract Betel Leaf waterNEWRNGMuthia HannisaNo ratings yet
- Jurnal Medical EmergenciesDocument11 pagesJurnal Medical EmergenciesMuthia HannisaNo ratings yet
- The Study of The Effect of Altering The Vertical Dimension of Occlusion On The Magnitude of Biting ForceDocument6 pagesThe Study of The Effect of Altering The Vertical Dimension of Occlusion On The Magnitude of Biting ForceMuthia HannisaNo ratings yet
- ScullyDocument1 pageScullyMuthia HannisaNo ratings yet
- Comparison of Bolton Analysis and Tooth SizeDocument5 pagesComparison of Bolton Analysis and Tooth SizeMuthia HannisaNo ratings yet
- Gow Gates Nerve BlockDocument4 pagesGow Gates Nerve BlockHudh HudNo ratings yet
- Gow Gates Nerve BlockDocument4 pagesGow Gates Nerve BlockHudh HudNo ratings yet
- InervasixxxDocument2 pagesInervasixxxMuthia HannisaNo ratings yet
- Praktikum Anatomi CompressedDocument23 pagesPraktikum Anatomi CompressedMuthia HannisaNo ratings yet
- Lirik Lagu ValentineDocument1 pageLirik Lagu ValentineMuthia HannisaNo ratings yet
- Impact of Empowerment On Toothbrushing and Diabetes ManagementDocument9 pagesImpact of Empowerment On Toothbrushing and Diabetes ManagementMuthia HannisaNo ratings yet
- Clinical Enzyme: Harliansyah, PH.D Head Dept. Biochemistry FKUY 2010Document20 pagesClinical Enzyme: Harliansyah, PH.D Head Dept. Biochemistry FKUY 2010Muthia HannisaNo ratings yet
- AsmaDocument9 pagesAsmaAnisa FazrinNo ratings yet
- Tugas EbmDocument8 pagesTugas EbmMuthia HannisaNo ratings yet
- Virology MCQDocument62 pagesVirology MCQGazi Shahinur Akter ShampaNo ratings yet
- Hand HygieneDocument8 pagesHand HygieneQwequ Gong AnanseNo ratings yet
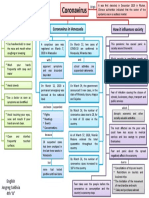
- Mapa Mental Coronavirus en InglesDocument1 pageMapa Mental Coronavirus en InglestavimayrNo ratings yet
- Chicken Pox InfographicsDocument1 pageChicken Pox InfographicsBIANCA PILNo ratings yet
- VaginitisDocument7 pagesVaginitisLei Ann FernandezNo ratings yet
- LimfadenitisDocument24 pagesLimfadenitisrahmah ningsihNo ratings yet
- Plot No.7G, Ground Floor, Opp. Graphite India, Telerad RXDX Healthcare PVT LTDDocument4 pagesPlot No.7G, Ground Floor, Opp. Graphite India, Telerad RXDX Healthcare PVT LTDSanjay TripathiNo ratings yet
- Yanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalityDocument1 pageYanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalitylisaNo ratings yet
- Dynamised Auto Therapy: Dr. G. Subash ChanderDocument12 pagesDynamised Auto Therapy: Dr. G. Subash ChanderMohammad AtaNo ratings yet
- Govt. of Himachal Pradesh: DEEPAK (Covid Pass No.: HP-2526572)Document2 pagesGovt. of Himachal Pradesh: DEEPAK (Covid Pass No.: HP-2526572)Vicky LakhanpalNo ratings yet
- Blood Grouping and Crosss MatchingDocument39 pagesBlood Grouping and Crosss MatchingDr. Pawan KumarNo ratings yet
- Hand Foot MouthDocument2 pagesHand Foot MouthBimantoro SaputroNo ratings yet
- The Intentional Murder of 'Canadian' First Nations For ProfitDocument2 pagesThe Intentional Murder of 'Canadian' First Nations For ProfitLuc MajnoNo ratings yet
- Jurnal 5MDocument8 pagesJurnal 5MNovi WulandariNo ratings yet
- Epidemiologi Penyakit TropisDocument36 pagesEpidemiologi Penyakit TropisHusein RahmatNo ratings yet
- GYNE 2.01a Lower Genital Tract Infections PDFDocument12 pagesGYNE 2.01a Lower Genital Tract Infections PDFMiguel Domingo100% (1)
- Coronavirus Will See Its End Soon, Say Renowned Astrologers - The WeekDocument4 pagesCoronavirus Will See Its End Soon, Say Renowned Astrologers - The WeekManuNo ratings yet
- MLT 107 Chapter 3 5 Infection Cont and QADocument29 pagesMLT 107 Chapter 3 5 Infection Cont and QACristina CunhaNo ratings yet
- General Cleaning Disinfecting Guide: Canine LeptospirosisDocument2 pagesGeneral Cleaning Disinfecting Guide: Canine LeptospirosisPATRICIA BROOKSNo ratings yet
- OnikomikosisDocument19 pagesOnikomikosisMerlyn Chrislia RumtheNo ratings yet
- AcinobacterDocument2 pagesAcinobacterAllyson Layaoen CollierNo ratings yet
- Pneumonia in Children What Is Pneumonia in Children?Document7 pagesPneumonia in Children What Is Pneumonia in Children?Sandra GabasNo ratings yet
- D&D 5e SkavenDocument1 pageD&D 5e SkavensyNo ratings yet
- Veterinary EctoparasitesDocument8 pagesVeterinary Ectoparasitesc3891446100% (1)
- Memo and Health Declaration Form FinalDocument5 pagesMemo and Health Declaration Form FinalALDINNo ratings yet
- Genitourinary Tract InfectionsDocument80 pagesGenitourinary Tract Infectionsraene_bautistaNo ratings yet
- Pathology MCQ - Infectious Disease PDFDocument5 pagesPathology MCQ - Infectious Disease PDFsilas mosha100% (2)
- FilariasisDocument13 pagesFilariasissarguss14100% (3)
- Smallpox Vaccines, Historical Review PDFDocument9 pagesSmallpox Vaccines, Historical Review PDFVijaykiran ReddyNo ratings yet
- Mask Order 2021Document1 pageMask Order 2021Leah MoreauNo ratings yet