You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- An Employee Benefits SMI/TISB ProductDocument37 pagesAn Employee Benefits SMI/TISB ProductAcik AchikNo ratings yet
- Satuan Biaya Rawat Inap Berdasarkan Golongan Sebab Penyakit Pada 84 Rumah Sakit Di Indonesia Tahun 2016Document10 pagesSatuan Biaya Rawat Inap Berdasarkan Golongan Sebab Penyakit Pada 84 Rumah Sakit Di Indonesia Tahun 2016Septa Ryan HidayatNo ratings yet
- Theresa Post Natal PackageDocument2 pagesTheresa Post Natal PackageSandra KohNo ratings yet
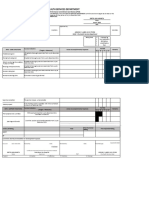
- City Health Services IPCR Performance ReviewDocument8 pagesCity Health Services IPCR Performance ReviewLiecel Valdez100% (2)
- Promotion Safe Med ChildrensDocument64 pagesPromotion Safe Med ChildrensAbdul khodir jaelani100% (1)
- Diabetes Case StudyDocument6 pagesDiabetes Case StudyDavid DeegbeNo ratings yet
- DyspepsiaDocument15 pagesDyspepsiaBo ChoiNo ratings yet
- VA Office of Inspector GeneralDocument46 pagesVA Office of Inspector Generalryan turbevilleNo ratings yet
- 93 Days: A Movie Review: The Story InvolvesDocument2 pages93 Days: A Movie Review: The Story InvolvesMelea Kristine RosalNo ratings yet
- Reflection: The Nursing Act of 1991 Protecting The Public Maria Claudia Esquivel Vasquez 805 349 214Document5 pagesReflection: The Nursing Act of 1991 Protecting The Public Maria Claudia Esquivel Vasquez 805 349 214api-283154156No ratings yet
- CLAIMING FACTS, VALUES, AND POLICIESDocument3 pagesCLAIMING FACTS, VALUES, AND POLICIESPrimo100% (2)
- Pediatric Musculoskeletal Summary For Osce ExamDocument53 pagesPediatric Musculoskeletal Summary For Osce Examopscurly100% (2)
- Feeding Plate: A Boon To Cleft Palate Child and Mother Too - Case ReportDocument10 pagesFeeding Plate: A Boon To Cleft Palate Child and Mother Too - Case ReportIJAR JOURNALNo ratings yet
- Effectiveness of nebulized N-acetylcysteine in treating children with acute bronchiolitisDocument4 pagesEffectiveness of nebulized N-acetylcysteine in treating children with acute bronchiolitisIvan VeriswanNo ratings yet
- Medical CertificateDocument126 pagesMedical CertificateAnonymous mummYD0% (1)
- ASA PS Classification System: Physical Status Definitions and ExamplesDocument2 pagesASA PS Classification System: Physical Status Definitions and ExamplesAnonymous 6iLtIrNo ratings yet
- Para LabDocument22 pagesPara LabClaudine DelacruzNo ratings yet
- LeaP Health G6 Week 1 Q3Document6 pagesLeaP Health G6 Week 1 Q3Mary Ann PerejaNo ratings yet
- Morocco - GHSDocument1 pageMorocco - GHSAli AmarNo ratings yet
- Effect of Emollient Therapy On Clinical Outcomes PDFDocument7 pagesEffect of Emollient Therapy On Clinical Outcomes PDFYESSICA MARCELA RODRIGUEZ QUECHONo ratings yet
- Brighter Futures - Orthodontic Endodontic Considerations Part 2Document4 pagesBrighter Futures - Orthodontic Endodontic Considerations Part 2Valonia IreneNo ratings yet
- Newborn Screening For Critical Congenital Heart Disease Using Pulse OximetryDocument20 pagesNewborn Screening For Critical Congenital Heart Disease Using Pulse OximetryHardian RakhmawardanaNo ratings yet
- The Protective Role of Maternal Immunization in Early LifeDocument15 pagesThe Protective Role of Maternal Immunization in Early LifeYasminNo ratings yet
- Jurnal Angkak Beras Merah DHFDocument11 pagesJurnal Angkak Beras Merah DHFAch ThungNo ratings yet
- Vanessa Hoos ResumeDocument3 pagesVanessa Hoos Resumeapi-533753716No ratings yet
- 2017 Boot Camp HandbookDocument98 pages2017 Boot Camp HandbookmyscribeNo ratings yet
- Rehabilitation Team Approach: Amputee PatientDocument35 pagesRehabilitation Team Approach: Amputee Patientwww_wadtulesh27No ratings yet
- Activity Intolerance Related To Decreased Cardiac Output, Due To EndocarditisDocument4 pagesActivity Intolerance Related To Decreased Cardiac Output, Due To EndocarditisJohn AlcantaraNo ratings yet
- Buser2000 PDFDocument10 pagesBuser2000 PDFArun PrasadNo ratings yet