You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2016-Brochure Umbilical CatheterDocument4 pages2016-Brochure Umbilical CatheterSuman MondalNo ratings yet
- Bilateral Refractive Amblyopia Treatment Study: ATS7 Protocol 5-24-04Document15 pagesBilateral Refractive Amblyopia Treatment Study: ATS7 Protocol 5-24-04samchu21No ratings yet
- Tugas Bahasa InggrisDocument4 pagesTugas Bahasa InggrisBerthy BlegurNo ratings yet
- Final Quiz PHI6 PDFDocument5 pagesFinal Quiz PHI6 PDFKenneth DayritNo ratings yet
- Feeling Your Baby Move ENGLISHDocument2 pagesFeeling Your Baby Move ENGLISHMehak ZNo ratings yet
- Pondichery DoctorsDocument2 pagesPondichery Doctorspriya selvaraj50% (2)
- InstrumentsDocument7 pagesInstrumentsOllet Athive NatacabNo ratings yet
- Echs EmpanelmentDocument316 pagesEchs EmpanelmentYudhvir SawhneyNo ratings yet
- Sulcus Vocalis Our Experience-DikonversiDocument5 pagesSulcus Vocalis Our Experience-DikonversiNuni SukindarNo ratings yet
- Need To Optimise Infant Feeding CounsellingDocument30 pagesNeed To Optimise Infant Feeding CounsellingfadnesNo ratings yet
- Roman Catholic: Lucena City, PHDocument4 pagesRoman Catholic: Lucena City, PHJennet RiveraNo ratings yet
- Obg Ward Teaching Infection ControlDocument37 pagesObg Ward Teaching Infection ControlbhavanaNo ratings yet
- Clopidogrel Bisulfate - PlavixDocument2 pagesClopidogrel Bisulfate - PlavixKristi WrayNo ratings yet
- Kidney TBDocument18 pagesKidney TBdrmsupriya091159No ratings yet
- Ambulatory HysterosDocument8 pagesAmbulatory Hysteroskomlanihou_890233161100% (1)
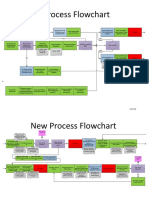
- New Process Flowchart CPOEDocument4 pagesNew Process Flowchart CPOELiza GeorgeNo ratings yet
- 1.2 Policies On Registration of A PatientDocument4 pages1.2 Policies On Registration of A PatientSwati Bajpai50% (2)
- AspergillosisDocument6 pagesAspergillosisDumitru PostolachiNo ratings yet
- Esophageal Perforation: Diagnostic Work-Up and Clinical Decision-Making in The First 24 HoursDocument7 pagesEsophageal Perforation: Diagnostic Work-Up and Clinical Decision-Making in The First 24 HourssyaifularisNo ratings yet
- 5 Suceessful Entrepreneur in MidwiferyDocument15 pages5 Suceessful Entrepreneur in MidwiferyKervin Lance Pascua0% (1)
- Ophthalmology: World Journal ofDocument5 pagesOphthalmology: World Journal ofRohamonangan TheresiaNo ratings yet
- TG 43Document9 pagesTG 43qftgaugeNo ratings yet
- Show Mom HowDocument20 pagesShow Mom HowWeldon Owen Publishing75% (4)
- 3 - Advances in The Diagnosis and Treatment of VasculitisDocument378 pages3 - Advances in The Diagnosis and Treatment of VasculitisAnonymous nGhxGKWXJr100% (1)
- Kaleidoscope Issue 73 - Coping With ChangeDocument70 pagesKaleidoscope Issue 73 - Coping With ChangeKaleidoscope: Exploring the Experience of Disability through Literature and the Fine Arts100% (1)
- WHO List of Basic Sources in English For A Medical Faculty LibraryDocument153 pagesWHO List of Basic Sources in English For A Medical Faculty LibraryLIS_141No ratings yet
- Government College of Nursing:, Jodhpur (Raj.)Document6 pagesGovernment College of Nursing:, Jodhpur (Raj.)priyankaNo ratings yet
- Morton's Metatarsalgia - Pathogenesis, Aetiology and Current ManagementDocument10 pagesMorton's Metatarsalgia - Pathogenesis, Aetiology and Current ManagementLikhit NayakNo ratings yet
- Cant Intubate Cant VentilateDocument6 pagesCant Intubate Cant Ventilatedannyromero2712No ratings yet
- Jurnal Oligohidramnion PDFDocument7 pagesJurnal Oligohidramnion PDFJuliana Dewi HadiNo ratings yet