You might also like
- Anatomia RiñonDocument28 pagesAnatomia RiñonNicol Irrazabal Tapia67% (3)
- Fase 2 - Definir El Plan de ActuaciónDocument10 pagesFase 2 - Definir El Plan de Actuaciónleidy lbañez50% (2)
- Coma MixedematosoDocument32 pagesComa MixedematosoAndrea Cruz marzanaNo ratings yet
- Myxedema Coma - UpToDateDocument14 pagesMyxedema Coma - UpToDateJulianaM.LanderasNo ratings yet
- Myxedema Coma - UpToDate PDFDocument7 pagesMyxedema Coma - UpToDate PDFPercy Hernandez RamosNo ratings yet
- Coma Mixedematoso - UpToDate PDFDocument15 pagesComa Mixedematoso - UpToDate PDFBecca MenciasNo ratings yet
- Comamixedematoso 141017174035 Conversion Gate02Document29 pagesComamixedematoso 141017174035 Conversion Gate02Guadalupe JojoNo ratings yet
- Coma MixedematosoDocument15 pagesComa MixedematosoAntonio SaavedraNo ratings yet
- Coma MixedematosoDocument12 pagesComa MixedematosoEmily PerezNo ratings yet
- Coma MixedematosoDocument8 pagesComa MixedematosoFrancisco Velez SaavedraNo ratings yet
- Enfermedad de AddisonDocument5 pagesEnfermedad de AddisonIdolo PasionNo ratings yet
- Enfermedad de AddisonDocument3 pagesEnfermedad de Addisondavidvilla0104No ratings yet
- EMERG. MÉDICAS III. Capitulo 3. Coma MixedematosoDocument12 pagesEMERG. MÉDICAS III. Capitulo 3. Coma MixedematosoGuillermo Sánchez VasquezNo ratings yet
- Coma MixedematosoDocument2 pagesComa MixedematosoViviana ValdiviaNo ratings yet
- HipotiroidismoDocument5 pagesHipotiroidismoJulio HernandezNo ratings yet
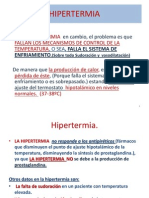
- HIPERTERMIADocument20 pagesHIPERTERMIAtefota100% (1)
- Rce 123 MDocument6 pagesRce 123 MMerci BaezNo ratings yet
- Coma MixedematosoDocument68 pagesComa MixedematosoOscar Quintana CordovaNo ratings yet
- HIPOTIROIDISMODocument8 pagesHIPOTIROIDISMOGabriela Gonzalez100% (1)
- EXPOSICIÓN - Biofísica (1) CertoDocument30 pagesEXPOSICIÓN - Biofísica (1) CertoLuana AlmeidaNo ratings yet
- Enfermedad de AddisonDocument10 pagesEnfermedad de AddisonIsamar Carolina AsuajesNo ratings yet
- HipotiroidismoDocument14 pagesHipotiroidismoJulieta GarridoNo ratings yet
- Trastornos de Las Glandulas SuprarrenalesDocument39 pagesTrastornos de Las Glandulas Suprarrenalesangie zevallosNo ratings yet
- Miocardiopatia Toxica o AcoholicaDocument30 pagesMiocardiopatia Toxica o AcoholicaJessi TorresNo ratings yet
- Urgencias Endocrinologicas Coma Mixedematoso Tormenta Tirotoxica IsaDocument8 pagesUrgencias Endocrinologicas Coma Mixedematoso Tormenta Tirotoxica IsaAilen Brett Cata'rNo ratings yet
- Tiroididtis de HashimotoDocument10 pagesTiroididtis de Hashimotopedro100% (1)
- Hiper e HipoDocument6 pagesHiper e Hiposthefany oleasNo ratings yet
- Hipotiroidismo (Tema 24)Document39 pagesHipotiroidismo (Tema 24)Yascila VilchezNo ratings yet
- Clasificacion de La HipotermiaDocument4 pagesClasificacion de La HipotermiaFernando Garcia GonzalezNo ratings yet
- Coma MixedematosoDocument6 pagesComa MixedematosoMaryuris ParraNo ratings yet
- Hipor e HipertiroidismoDocument44 pagesHipor e HipertiroidismoJesús Rodríguez MundacaNo ratings yet
- HIPOTERMIADocument3 pagesHIPOTERMIAalessandraNo ratings yet
- Hipotermia Un Peligro en Todas Las EstacionesDocument4 pagesHipotermia Un Peligro en Todas Las Estacionesprincejor13No ratings yet
- Etiología Del HipotiroidismoDocument6 pagesEtiología Del HipotiroidismoSandy Diaz AvilaNo ratings yet
- HIPOTIROIDISMODocument7 pagesHIPOTIROIDISMOalexandraNo ratings yet
- 80 Urgencias EndocrinológicasDocument8 pages80 Urgencias EndocrinológicasAillyne ArceNo ratings yet
- Endocrino 2.0Document36 pagesEndocrino 2.0LorePaz100% (1)
- Hiponatremia Resumen FisiopatologiaDocument4 pagesHiponatremia Resumen FisiopatologiaIvanna MendozaNo ratings yet
- Endocrino IDocument18 pagesEndocrino IReinalda Campuzano MendozaNo ratings yet
- Hipotiroidismo E HipertiroidismoDocument4 pagesHipotiroidismo E HipertiroidismoAlberto E.No ratings yet
- Disfunción TiroideaDocument6 pagesDisfunción TiroideaJHOSELYNENo ratings yet
- HipertiroidismoDocument34 pagesHipertiroidismoCami LaureNo ratings yet
- U3. TrastornosDocument147 pagesU3. TrastornosAndrea Drew ReyesNo ratings yet
- TermoregulacionDocument1 pageTermoregulacionRicardo CastroNo ratings yet
- Hipotiroidismo Luis UpeDocument36 pagesHipotiroidismo Luis UpeLuis Manuel Cabrera LibreroNo ratings yet
- HipotiroidismoDocument5 pagesHipotiroidismolinkerikNo ratings yet
- Coma MixedematosoDocument3 pagesComa MixedematosoSofia MoralesNo ratings yet
- HipotiroidismoDocument8 pagesHipotiroidismoChristian QuinterosNo ratings yet
- Trastornos Del Sist ENDOCRINODocument12 pagesTrastornos Del Sist ENDOCRINOjossy andersonNo ratings yet
- Sindrome Febril HUCDocument8 pagesSindrome Febril HUCRafael Andrés Hanssen HargitayNo ratings yet
- Alteracion y Regulacion de La Temperatura y FiebreDocument4 pagesAlteracion y Regulacion de La Temperatura y FiebreJosselin Joyce Meléndez HernándezNo ratings yet
- Signos VitalesDocument9 pagesSignos VitalesDaniel Adrián Conei ValenciaNo ratings yet
- 4 - TermorregulacionDocument19 pages4 - TermorregulacionDaniela Castillo GonzálezNo ratings yet
- HipotermiaDocument2 pagesHipotermiaYdeli DetanNo ratings yet
- Caso Clínico #1Document11 pagesCaso Clínico #1LUIS MANUEL ORTIZ DE LEONNo ratings yet
- HIPOTIROIDISMODocument22 pagesHIPOTIROIDISMODeyvi Villarroel CossioNo ratings yet
- 110 Hipotermia 02 FinalDocument5 pages110 Hipotermia 02 FinalEuyi EluNo ratings yet
- Lesion Por FrioDocument14 pagesLesion Por FrioYamil GomezNo ratings yet
- HM 2Document31 pagesHM 2api-231684004No ratings yet
- Urgencias TiroideasDocument9 pagesUrgencias TiroideasXochil RmzNo ratings yet
- Tratando Con El Dolor De Espalda: Aprende más sobre el dolor de espalda y su relación con la esclerosis múltiple, el herpes simple y otros malesFrom EverandTratando Con El Dolor De Espalda: Aprende más sobre el dolor de espalda y su relación con la esclerosis múltiple, el herpes simple y otros malesRating: 5 out of 5 stars5/5 (2)
- Uso del Cannabis en la epilepsia refractaria infantilFrom EverandUso del Cannabis en la epilepsia refractaria infantilNo ratings yet
- Evidencia de Las Ondas de ChoqueDocument7 pagesEvidencia de Las Ondas de ChoqueamexatoNo ratings yet
- Clima Organizacional en El Sector SaludDocument12 pagesClima Organizacional en El Sector SaludamexatoNo ratings yet
- Bloqueo FacetarioDocument6 pagesBloqueo FacetarioamexatoNo ratings yet
- DL 1440Document16 pagesDL 1440Elvis Huaysara R.No ratings yet
- Compendio de Legislacion en Salud - 2009Document544 pagesCompendio de Legislacion en Salud - 2009Jose NestaresNo ratings yet
- Facturacion InternacionalDocument9 pagesFacturacion InternacionalamexatoNo ratings yet
- Guía Técnica para La Categorización de Establecimientos Del Sector SaludDocument24 pagesGuía Técnica para La Categorización de Establecimientos Del Sector Saludamexato0% (1)
- Criterios de Uso de HemoderivadosDocument31 pagesCriterios de Uso de HemoderivadosamexatoNo ratings yet
- RM539-2006 Retinopatía de La Prematuridad GPCDocument27 pagesRM539-2006 Retinopatía de La Prematuridad GPCLisbeth Quispe PeñaNo ratings yet
- Guías Nacionales de Atención Integral de La Salud Sexual y ReproductivaDocument273 pagesGuías Nacionales de Atención Integral de La Salud Sexual y ReproductivaStephani Luna Solís100% (1)
- RN Sano y EnfermoDocument131 pagesRN Sano y EnfermoTaNu GutierrezNo ratings yet
- APUNTES DE SALUD Y MEDICINA DEL PERU ANTIGUO Por HUGO A DEJO BUSTIOS PDFDocument288 pagesAPUNTES DE SALUD Y MEDICINA DEL PERU ANTIGUO Por HUGO A DEJO BUSTIOS PDFJaime Jose Arias Congrains100% (1)
- Guia de Práctica Clinica de Sepsis en UCI MINSADocument17 pagesGuia de Práctica Clinica de Sepsis en UCI MINSAamexatoNo ratings yet
- Informe Final2Document8 pagesInforme Final2amexatoNo ratings yet
- GPC Manejo de La Erc Enero2010Document65 pagesGPC Manejo de La Erc Enero2010Alexander Callapiña100% (1)
- Norma de Emergencia 2001 PDFDocument19 pagesNorma de Emergencia 2001 PDFamexatoNo ratings yet
- Efecto Del Extracto de Hoja de Coca en RatonesDocument49 pagesEfecto Del Extracto de Hoja de Coca en RatonesamexatoNo ratings yet
- Carro RojoDocument7 pagesCarro RojoJennifer CalderónNo ratings yet
- II Exámen de Biología 2Document10 pagesII Exámen de Biología 2Oskitar 123No ratings yet
- Capítulo 5. CarbamatosDocument8 pagesCapítulo 5. CarbamatosJeanethe CastilloNo ratings yet
- SuicidioDocument27 pagesSuicidioBondis EmeNo ratings yet
- Ejercicios para Facilitar La Marcha en La EnfermedadDocument14 pagesEjercicios para Facilitar La Marcha en La EnfermedadNicolas Espinoza ConstanzoNo ratings yet
- Tesis Ana LeyvaDocument53 pagesTesis Ana LeyvaFidel Vladimiro67% (3)
- Bombas de InfusionDocument7 pagesBombas de InfusionDiana MartinezNo ratings yet
- Gasometría Sanguínea y Trastornos Ácido-Base - Sopemi 2022 (1) IvisDocument83 pagesGasometría Sanguínea y Trastornos Ácido-Base - Sopemi 2022 (1) IvisIvis GuavaraNo ratings yet
- Sistema InmuneDocument25 pagesSistema InmuneMaribel AlvearNo ratings yet
- Guia Salud Personas Con Discapacidad en La Salud Rural - MODULO 2Document21 pagesGuia Salud Personas Con Discapacidad en La Salud Rural - MODULO 2Dan Dan Sr.No ratings yet
- Enfermedades Por Agentes FisicosDocument39 pagesEnfermedades Por Agentes FisicosalfredoairNo ratings yet
- DOF - Diario Oficial de La Federación 12Document3 pagesDOF - Diario Oficial de La Federación 12Hugo Alberto Nolasco VazquezNo ratings yet
- 1.aps IntroduccionDocument24 pages1.aps IntroduccionCarmen Luisa Escobar AstrelliNo ratings yet
- Normas de Bioseguridad en La Practica Odontologica PDFDocument9 pagesNormas de Bioseguridad en La Practica Odontologica PDFkateNo ratings yet
- El Optimismo Como Factor ProtectorDocument4 pagesEl Optimismo Como Factor ProtectorMiriam Agudo MarinNo ratings yet
- Cuestionarios de InmunoDocument10 pagesCuestionarios de InmunojoelNo ratings yet
- La Práctica RespiratoriaDocument10 pagesLa Práctica RespiratoriaCarolina Yohana Manríquez AcuñaNo ratings yet
- Incapacidad 2Document2 pagesIncapacidad 2Jhon Duarte100% (1)
- Modelo de Consentimiento y Asentimiento InformadoDocument5 pagesModelo de Consentimiento y Asentimiento InformadoEdson Huansi AndyNo ratings yet
- Tejido Conjuntivo EspecializadoDocument64 pagesTejido Conjuntivo EspecializadoMaria LauraNo ratings yet
- Manual Toma Presion Yuwell YE670D TopMedicDocument23 pagesManual Toma Presion Yuwell YE670D TopMedicLourdes CordobaNo ratings yet
- Guia CartaDocument3 pagesGuia Cartacaro veasNo ratings yet
- MACROLIDOSDocument3 pagesMACROLIDOSXimena MilenaNo ratings yet
- Art Agtr1 Nefrologia 2Document16 pagesArt Agtr1 Nefrologia 2Irene MNo ratings yet
- Resumen Unidad I y II Clinica CompletoDocument53 pagesResumen Unidad I y II Clinica CompletoGabi PalaciosNo ratings yet
- LudopatíaDocument37 pagesLudopatíaNicolás Rodríguez Del RealNo ratings yet
- Especificaciones Del Sistema DigestivoDocument3 pagesEspecificaciones Del Sistema Digestivorudy_batenNo ratings yet
- Perma-Modelo para Ser FelizDocument4 pagesPerma-Modelo para Ser FelizJota RuanoNo ratings yet