You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Meat Plant FeasabilityDocument115 pagesMeat Plant FeasabilityCh WaqasNo ratings yet
- Method StatementDocument29 pagesMethod StatementZakwan Hisyam100% (1)
- Pe 3 Syllabus - GymnasticsDocument7 pagesPe 3 Syllabus - GymnasticsLOUISE DOROTHY PARAISO100% (1)
- Art of Facing InterviewsDocument15 pagesArt of Facing Interviewskrish_cvr2937100% (2)
- General Chemistry 2 Quarter 4 - Week 4 Module 4: PH of Buffer SolutionsDocument12 pagesGeneral Chemistry 2 Quarter 4 - Week 4 Module 4: PH of Buffer SolutionsHazel EncarnacionNo ratings yet
- Chemical Engineering Projects List For Final YearDocument2 pagesChemical Engineering Projects List For Final YearRajnikant Tiwari67% (6)
- Lichens - Naturally Scottish (Gilbert 2004) PDFDocument46 pagesLichens - Naturally Scottish (Gilbert 2004) PDF18Delta100% (1)
- Doctors ListDocument212 pagesDoctors ListSaranya Chandrasekar33% (3)
- Dr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFDocument72 pagesDr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFagnesspratiwiNo ratings yet
- 193 Iajps193092020-1 PDFDocument8 pages193 Iajps193092020-1 PDFiajpsNo ratings yet
- 193 Iajps193092020-1 PDFDocument8 pages193 Iajps193092020-1 PDFiajpsNo ratings yet
- Pharmaceutical Sciences: Pregnancy Outcomes of Covid-19 Positive Patients A Systematic Review of LiteratureDocument6 pagesPharmaceutical Sciences: Pregnancy Outcomes of Covid-19 Positive Patients A Systematic Review of LiteratureiajpsNo ratings yet
- 196 Iajps196092020 PDFDocument4 pages196 Iajps196092020 PDFiajpsNo ratings yet
- 197 Iajps197092020 PDFDocument5 pages197 Iajps197092020 PDFiajpsNo ratings yet
- 194 Iajps194092020 PDFDocument7 pages194 Iajps194092020 PDFiajpsNo ratings yet
- 195 Iajps195092020 PDFDocument5 pages195 Iajps195092020 PDFiajpsNo ratings yet
- 46 Iajps46102020Document7 pages46 Iajps46102020iajpsNo ratings yet
- 40 Iajps40102020Document4 pages40 Iajps40102020iajpsNo ratings yet
- 191 Iajps191092020Document8 pages191 Iajps191092020iajpsNo ratings yet
- Pharmaceutical Sciences: Flipping Impacts of Middle School Laboratory in Health School EducationDocument4 pagesPharmaceutical Sciences: Flipping Impacts of Middle School Laboratory in Health School EducationiajpsNo ratings yet
- 50 Iajps50102020Document13 pages50 Iajps50102020iajpsNo ratings yet
- 192 Iajps192092020 PDFDocument5 pages192 Iajps192092020 PDFiajpsNo ratings yet
- Pharmaceutical Sciences: The Impact of Ox Like Lactoferrin (BLF) On Prevention of The Diarrhoea in YoungstersDocument7 pagesPharmaceutical Sciences: The Impact of Ox Like Lactoferrin (BLF) On Prevention of The Diarrhoea in YoungstersiajpsNo ratings yet
- Pharmaceutical Sciences: Observation of Metabolism According To The Growth Hormone Control in Mayo Hospital LahoreDocument6 pagesPharmaceutical Sciences: Observation of Metabolism According To The Growth Hormone Control in Mayo Hospital LahoreiajpsNo ratings yet
- Pharmaceutical Sciences: Urinary Sodium and Potassium Discharge and Danger of Hypertension in Pakistani PopulationDocument4 pagesPharmaceutical Sciences: Urinary Sodium and Potassium Discharge and Danger of Hypertension in Pakistani PopulationiajpsNo ratings yet
- 44 Iajps44102020Document4 pages44 Iajps44102020iajpsNo ratings yet
- Pharmaceutical Sciences: Study To Determine The Pattern of Primary Glomerulonephritis in PakistanDocument5 pagesPharmaceutical Sciences: Study To Determine The Pattern of Primary Glomerulonephritis in PakistaniajpsNo ratings yet
- Pharmaceutical Sciences: Management of Proximal Ureteric Stone (10 - 15 MM Size) Via Urs & EswlDocument6 pagesPharmaceutical Sciences: Management of Proximal Ureteric Stone (10 - 15 MM Size) Via Urs & EswliajpsNo ratings yet
- 35 Iajps35102020Document4 pages35 Iajps35102020iajpsNo ratings yet
- Pharmaceutical Sciences: A Young Male With Splenic Vein and SMV Thrombosis and Jak 22 MutationDocument12 pagesPharmaceutical Sciences: A Young Male With Splenic Vein and SMV Thrombosis and Jak 22 MutationiajpsNo ratings yet
- 42 Iajps42102020Document8 pages42 Iajps42102020iajpsNo ratings yet
- Pharmaceutical Sciences: Psychophysiological Features of Students Aerobic Abilities and Maintaining A Healthy LifestyleDocument6 pagesPharmaceutical Sciences: Psychophysiological Features of Students Aerobic Abilities and Maintaining A Healthy LifestyleiajpsNo ratings yet
- Pharmaceutical Sciences: Cognitive Schemes For Clinical Diagnostic Reasoning by Medical StudentsDocument8 pagesPharmaceutical Sciences: Cognitive Schemes For Clinical Diagnostic Reasoning by Medical StudentsiajpsNo ratings yet
- Pharmaceutical Sciences: Teneligliptin Induced Persistent DiarrheaDocument3 pagesPharmaceutical Sciences: Teneligliptin Induced Persistent DiarrheaiajpsNo ratings yet
- Pharmaceutical SciencesDocument5 pagesPharmaceutical SciencesiajpsNo ratings yet
- 37 Iajps37102020Document9 pages37 Iajps37102020iajpsNo ratings yet
- 34 Iajps34102020Document7 pages34 Iajps34102020iajpsNo ratings yet
- 33 Iajps33102020Document6 pages33 Iajps33102020iajpsNo ratings yet
- Pharmaceutical Sciences: Clinical Manifestations of Sars-Cov-2 (Covid19)Document5 pagesPharmaceutical Sciences: Clinical Manifestations of Sars-Cov-2 (Covid19)iajpsNo ratings yet
- Benzil PDFDocument5 pagesBenzil PDFAijaz NawazNo ratings yet
- Mid Day Meal Scheme-Case Study of BiharDocument4 pagesMid Day Meal Scheme-Case Study of BiharKaran singh RautelaNo ratings yet
- Comprehensive Safe Hospital FrameworkDocument12 pagesComprehensive Safe Hospital FrameworkEbby OktaviaNo ratings yet
- Pioneer PDP 5071 5070pu Arp 3354Document219 pagesPioneer PDP 5071 5070pu Arp 3354Dan Prewitt100% (1)
- Mil STD 792fDocument13 pagesMil STD 792fdoradoanNo ratings yet
- Starkville Dispatch Eedition 9-10-20Document12 pagesStarkville Dispatch Eedition 9-10-20The DispatchNo ratings yet
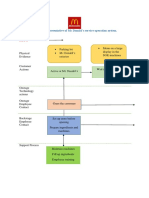
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 pagesBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNo ratings yet
- IsoTherming® Hydroprocessing TechnologyDocument4 pagesIsoTherming® Hydroprocessing Technologyromi moriNo ratings yet
- E61 DiagramDocument79 pagesE61 Diagramthanes1027No ratings yet
- Education in America: The Dumbing Down of The U.S. Education SystemDocument4 pagesEducation in America: The Dumbing Down of The U.S. Education SystemmiichaanNo ratings yet
- Chapter 2 and 3 ImmunologyDocument16 pagesChapter 2 and 3 ImmunologyRevathyNo ratings yet
- Solar Refrigeration: Prepared by M.DevakumarDocument21 pagesSolar Refrigeration: Prepared by M.DevakumarEasy StudyNo ratings yet
- Terminologi AnatomiaDocument49 pagesTerminologi AnatomiaLuluk QurrataNo ratings yet
- G103 Remov Waste Dust Extraction UnitDocument2 pagesG103 Remov Waste Dust Extraction UnitJoseCRomeroNo ratings yet
- Interviewing Skill Workshop (KAU)Document54 pagesInterviewing Skill Workshop (KAU)DrKomal KhalidNo ratings yet
- Installing Touareg R5 CamshaftDocument1 pageInstalling Touareg R5 CamshaftSarunas JurciukonisNo ratings yet
- Wisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseDocument3 pagesWisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseTMJ4 NewsNo ratings yet
- Flusarc 36: Gas-Insulated SwitchgearDocument76 pagesFlusarc 36: Gas-Insulated SwitchgearJoey Real CabalidaNo ratings yet
- Pantera 900Document3 pagesPantera 900Tuan Pham AnhNo ratings yet
- Libro Resumenes 2012Document735 pagesLibro Resumenes 2012fdobonat613100% (2)
- Arsenal Strength Catalog 6.2-1Document41 pagesArsenal Strength Catalog 6.2-1Mohammed NavedNo ratings yet