You might also like
- English Vocabulary 2: No. Nama FotoDocument8 pagesEnglish Vocabulary 2: No. Nama Fotofiora.ladesvitaNo ratings yet
- Mahjoob2014 PDFDocument5 pagesMahjoob2014 PDFfiora.ladesvitaNo ratings yet
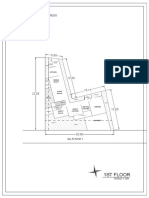
- 1St Floor: House On Paus Schematic Plan ProgressDocument2 pages1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaNo ratings yet
- Smooth Sailing - Navigating The Sea of Law Applicable To The CruiDocument35 pagesSmooth Sailing - Navigating The Sea of Law Applicable To The Cruifiora.ladesvitaNo ratings yet
- Vocab Coco 2Document7 pagesVocab Coco 2fiora.ladesvitaNo ratings yet
- English Vocabulary: No. Nama FotoDocument7 pagesEnglish Vocabulary: No. Nama Fotofiora.ladesvitaNo ratings yet
- Des An Jose 2019Document6 pagesDes An Jose 2019fiora.ladesvitaNo ratings yet
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyDocument10 pagesDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaNo ratings yet
- Quat Trin 2006Document10 pagesQuat Trin 2006fiora.ladesvitaNo ratings yet
- Gibson 2010Document19 pagesGibson 2010fiora.ladesvitaNo ratings yet
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocument12 pagesChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaNo ratings yet
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyDocument11 pagesSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaNo ratings yet
- F374W1M2L5G52563 FirstDocument1 pageF374W1M2L5G52563 Firstfiora.ladesvitaNo ratings yet
- Abdul Kadir 2016Document7 pagesAbdul Kadir 2016fiora.ladesvitaNo ratings yet
- ID Perbandingan Kualitas Hidup Pasien Gagal PDFDocument9 pagesID Perbandingan Kualitas Hidup Pasien Gagal PDFAlawiyahRasyaNo ratings yet
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocument12 pagesChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaNo ratings yet
- Lalla 2008Document17 pagesLalla 2008fiora.ladesvitaNo ratings yet
- Quat Trin 2006Document10 pagesQuat Trin 2006fiora.ladesvitaNo ratings yet
- G15 v03 ED Design Guidelines Dec-14Document77 pagesG15 v03 ED Design Guidelines Dec-14gracegozaliNo ratings yet
- Managing Oral Mucositis Oral Health July 2015Document4 pagesManaging Oral Mucositis Oral Health July 2015fiora.ladesvitaNo ratings yet
- Full TextDocument127 pagesFull Textfiora.ladesvitaNo ratings yet
- Lalla 2008Document17 pagesLalla 2008fiora.ladesvitaNo ratings yet
- Abdul Kadir 2016Document7 pagesAbdul Kadir 2016fiora.ladesvitaNo ratings yet
- Medicalscience: EcancerDocument7 pagesMedicalscience: Ecancerfiora.ladesvitaNo ratings yet
- Assessment Rating ScaleDocument8 pagesAssessment Rating Scalefiora.ladesvitaNo ratings yet
- Ni Hms 544150Document15 pagesNi Hms 544150fiora.ladesvitaNo ratings yet
- Ambulatory Care Nursing: Coming Soon!Document16 pagesAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaNo ratings yet
- 2015 Conference 10Document11 pages2015 Conference 10fiora.ladesvitaNo ratings yet
- Anderson2004 PDFDocument7 pagesAnderson2004 PDFfiora.ladesvitaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Raj Yoga ReportDocument17 pagesRaj Yoga ReportSweaty Sunny50% (2)
- Posture of EcstasyDocument1 pagePosture of EcstasyJonathanNo ratings yet
- Astro PhotoDocument12 pagesAstro PhotoPavelNo ratings yet
- Intelligent Control LED Integrated Light Source: Features and BenefitsDocument6 pagesIntelligent Control LED Integrated Light Source: Features and BenefitsRazvy StoianNo ratings yet
- Finding Answers Through Data Collection: Data Collection Procedure and Skills Using Varied InstrumentsDocument4 pagesFinding Answers Through Data Collection: Data Collection Procedure and Skills Using Varied InstrumentsJude BautistaNo ratings yet
- Ais For PROTONDocument18 pagesAis For PROTONAfaf RadziNo ratings yet
- Voyagers: Game of Flames (Book 2) by Robin WassermanDocument35 pagesVoyagers: Game of Flames (Book 2) by Robin WassermanRandom House KidsNo ratings yet
- Chapter One 1.1. Background of The Study: Iloilo City's Heritage Tourist Destinations Are Worth Keeping ForDocument2 pagesChapter One 1.1. Background of The Study: Iloilo City's Heritage Tourist Destinations Are Worth Keeping ForCrisNo ratings yet
- 2011catalog p48-55 PDFDocument4 pages2011catalog p48-55 PDFRoina Flores100% (1)
- How GE Is Disrupting ItselfDocument2 pagesHow GE Is Disrupting ItselfAdithya PrabuNo ratings yet
- ESCL-QSP-005, Corrective Action ProcedureDocument6 pagesESCL-QSP-005, Corrective Action Procedureadiqualityconsult100% (1)
- Leopold, L. T. 1968 Hydrology For Urban Planning - A Guide Book On TheDocument26 pagesLeopold, L. T. 1968 Hydrology For Urban Planning - A Guide Book On TheFiguraDesfiguraNo ratings yet
- Marzano's Compendium: Acknowledging Adherence To Rules and ProceduresDocument28 pagesMarzano's Compendium: Acknowledging Adherence To Rules and ProceduresClaudia VelascoNo ratings yet
- 749481Document3 pages749481PAULSON K ANTONY 17BEC1147100% (1)
- NCI Operations Manual June 28Document225 pagesNCI Operations Manual June 28bile_driven_opus100% (1)
- Kcpe Maths Made Familiar QNSDocument96 pagesKcpe Maths Made Familiar QNSGodwin Ayieko100% (1)
- SRS APO Panel ReadmeDocument25 pagesSRS APO Panel ReadmeLiz Minmey Flores FloresNo ratings yet
- Kimia Percubaan SPM 2009 Kertas 1, 2, 3 MRSMDocument68 pagesKimia Percubaan SPM 2009 Kertas 1, 2, 3 MRSMCarolyn Chang Boon ChuiNo ratings yet
- Meditatons of Maharishi Mahesh Yogi - MAHARISHI MAHESH YOGIDocument139 pagesMeditatons of Maharishi Mahesh Yogi - MAHARISHI MAHESH YOGIAshwani Kumar100% (2)
- What Are You Going To Do Today?: Learning ObjectivesDocument10 pagesWhat Are You Going To Do Today?: Learning ObjectivesMaryantiNo ratings yet
- Data Mining in The Insurance Industry - Solving Business Problems Using SAS Enterprise Miner SoftwareDocument20 pagesData Mining in The Insurance Industry - Solving Business Problems Using SAS Enterprise Miner SoftwareShehan1No ratings yet
- CH 12Document76 pagesCH 12Christian JeremiaNo ratings yet
- Yameena Rashid: ObjectivesDocument2 pagesYameena Rashid: ObjectivesMisbhasaeedaNo ratings yet
- Practice Types of SentenceDocument6 pagesPractice Types of SentenceTrần Hồ Quỳnh HươngNo ratings yet
- Facebook Romanian Translation Style GuideDocument20 pagesFacebook Romanian Translation Style GuideLeonNo ratings yet
- Sir Josiah Stamp, The Science of Social AdjustmentDocument191 pagesSir Josiah Stamp, The Science of Social Adjustmentmaivin2No ratings yet
- BhishmaDocument6 pagesBhishmaHarsh SoniNo ratings yet
- Servomotor PptsDocument26 pagesServomotor Pptsjasdeep_kour236066No ratings yet
- Using Keyframe SynfigDocument1 pageUsing Keyframe SynfigNdandungNo ratings yet