You might also like
- Determining Time of Death Methods and FactorsDocument10 pagesDetermining Time of Death Methods and FactorsJack GuccioneNo ratings yet
- Sporzon! Olympic Weightlifting Barbell, 700 LB Capacity, Silver Sports & OutdoorsDocument1 pageSporzon! Olympic Weightlifting Barbell, 700 LB Capacity, Silver Sports & OutdoorsJack GuccioneNo ratings yet
- UCI Health Neuropsychiatric Center UCI Health Orange County, CADocument1 pageUCI Health Neuropsychiatric Center UCI Health Orange County, CAJack GuccioneNo ratings yet
- Recreation Park 18 Golf Course - Online BookingDocument1 pageRecreation Park 18 Golf Course - Online BookingJack GuccioneNo ratings yet
- Ninjas Guide Remote LearningDocument197 pagesNinjas Guide Remote LearningJack GuccioneNo ratings yet
- GROSSING TEMPLATESDocument51 pagesGROSSING TEMPLATESJack GuccioneNo ratings yet
- Fishing Net Industrial - Google SearchDocument1 pageFishing Net Industrial - Google SearchJack GuccioneNo ratings yet
- At Your Service Online Sign inDocument1 pageAt Your Service Online Sign inJack GuccioneNo ratings yet
- Get Your Ascent Cycles Memorabilia!Document1 pageGet Your Ascent Cycles Memorabilia!Jack GuccioneNo ratings yet
- Robert F. Kennedy, Jr. - Google SearchDocument1 pageRobert F. Kennedy, Jr. - Google SearchJack GuccioneNo ratings yet
- Anaheim Hills Golf Course - Online BookingDocument1 pageAnaheim Hills Golf Course - Online BookingJack GuccioneNo ratings yet
- Election Results - Google SearchDocument1 pageElection Results - Google SearchJack GuccioneNo ratings yet
- Goals and Objectives of ICU-1Document3 pagesGoals and Objectives of ICU-1Jack GuccioneNo ratings yet
- BMW Fuel Tank Leak Module Extended Warranty - RedactedDocument3 pagesBMW Fuel Tank Leak Module Extended Warranty - RedactedJack GuccioneNo ratings yet
- The Relationship Between Primary Care, Income Inequality, and Mortality in US States, 1980-1995Document11 pagesThe Relationship Between Primary Care, Income Inequality, and Mortality in US States, 1980-1995Jack GuccioneNo ratings yet
- Hypersensitivity To Nickel in A Patient Treated With Coil Embolization For Pelvic Congestion SyndromeDocument3 pagesHypersensitivity To Nickel in A Patient Treated With Coil Embolization For Pelvic Congestion SyndromeJack GuccioneNo ratings yet
- Family Medicine Textbook Notes PDFDocument174 pagesFamily Medicine Textbook Notes PDFJack GuccioneNo ratings yet
- Request For Interviewing Time Off (10-14)Document1 pageRequest For Interviewing Time Off (10-14)Jack GuccioneNo ratings yet
- CAT Student Worksheet FormDocument2 pagesCAT Student Worksheet FormJack GuccioneNo ratings yet
- Recognizing and Reducing Unconscious Bias in Healthcare: Patricia Flynn, PH.D., M.P.HDocument16 pagesRecognizing and Reducing Unconscious Bias in Healthcare: Patricia Flynn, PH.D., M.P.HJack Guccione100% (1)
- Patient Tracker OME PDFDocument2 pagesPatient Tracker OME PDFJack GuccioneNo ratings yet
- Patient Tracker OME PDFDocument2 pagesPatient Tracker OME PDFJack GuccioneNo ratings yet
- Read MeDocument1 pageRead MeJack GuccioneNo ratings yet
- Metal-Induced Generalized Pruriginous Dermatitis and Endovascular SurgeryDocument6 pagesMetal-Induced Generalized Pruriginous Dermatitis and Endovascular SurgeryJack GuccioneNo ratings yet
- Med H&P TemplateDocument2 pagesMed H&P TemplatehellayeahNo ratings yet
- Uwise HYDocument3 pagesUwise HYJack GuccioneNo ratings yet
- Week5 - Quiz5 - CLIPP CasesDocument1 pageWeek5 - Quiz5 - CLIPP CasesJack GuccioneNo ratings yet
- NBME CMS Forms NotesDocument4 pagesNBME CMS Forms NotesJack Guccione100% (7)
- Usmle RX Hy NotesDocument1 pageUsmle RX Hy NotesJack GuccioneNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cavalry Journal, Volume 2, Nos. 4, 5, 6 & 7Document222 pagesCavalry Journal, Volume 2, Nos. 4, 5, 6 & 7"Rufus"No ratings yet
- Eloqua Landing Page Optimization and Best PracticesDocument42 pagesEloqua Landing Page Optimization and Best Practicessidhartha883No ratings yet
- Falcon Private BankDocument64 pagesFalcon Private BankChevy ShopNo ratings yet
- Spring Ldap ReferenceDocument58 pagesSpring Ldap Referenceskd_juNo ratings yet
- Safety and Security Co-Analyses: A Systematic Literature ReviewDocument12 pagesSafety and Security Co-Analyses: A Systematic Literature ReviewWaren L ParingitNo ratings yet
- Manual Hampton Bay Ceiling FanDocument16 pagesManual Hampton Bay Ceiling FanRafael GarciaNo ratings yet
- Lead SOC Manager Job DescriptionDocument2 pagesLead SOC Manager Job DescriptionsplfriendsNo ratings yet
- Slashnext Targeted Phishing Defense DatasheetDocument2 pagesSlashnext Targeted Phishing Defense DatasheetNasirNo ratings yet
- ECall LetterDocument2 pagesECall LetterGiriraj DeoraNo ratings yet
- MylifeDocument2 pagesMylifejohn sparksNo ratings yet
- BSOD - System Error Codes (English Version)Document98 pagesBSOD - System Error Codes (English Version)Mohamad Ridzuan Abdul MajidNo ratings yet
- QR Code DetailsDocument2 pagesQR Code DetailsRb143No ratings yet
- Step-By-Step - Adding A Windows Server 2012 Domain Controller To An Existing Windows Server 2003 Network PDFDocument13 pagesStep-By-Step - Adding A Windows Server 2012 Domain Controller To An Existing Windows Server 2003 Network PDFEmilio MartinezNo ratings yet
- Junos Release Notes 12.1Document235 pagesJunos Release Notes 12.1omo-obaNo ratings yet
- Reliance Industries Limited: Hazira Manufacturing DivisionDocument20 pagesReliance Industries Limited: Hazira Manufacturing DivisionTracy WhiteNo ratings yet
- Challenges and New Directions For AI and Hardware SecurityDocument4 pagesChallenges and New Directions For AI and Hardware SecurityHarrishNo ratings yet
- RFID BENEFITSDocument12 pagesRFID BENEFITSrz2491No ratings yet
- DRMDocument54 pagesDRMthe_tigdraNo ratings yet
- Annexure 7 - Extract of Annual Return: Form No. MGT-9 Registration and Other DetailsDocument1 pageAnnexure 7 - Extract of Annual Return: Form No. MGT-9 Registration and Other DetailsJittu Elsa JoseNo ratings yet
- MegaMek Scenario DescriptionsDocument5 pagesMegaMek Scenario Descriptionsrgamer7No ratings yet
- The Untold Story of Silk Road, Part 1Document42 pagesThe Untold Story of Silk Road, Part 1HeartwalkerNo ratings yet
- 1SDA066549R1 A2b 250 TMF 160 1600 3p F FDocument2 pages1SDA066549R1 A2b 250 TMF 160 1600 3p F FYa ZenNo ratings yet
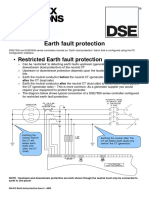
- 056-019 Earth Fault Protection PDFDocument2 pages056-019 Earth Fault Protection PDFmigas_migue2856No ratings yet
- SADlab 3 - 2005103Document2 pagesSADlab 3 - 2005103Rahul ShahNo ratings yet
- FFDocument4 pagesFFMohd AsifNo ratings yet
- GSM Sms Eth ControllerDocument24 pagesGSM Sms Eth ControllerAleksandra DomazetoskaNo ratings yet
- Enhancing Forest Fires Preparedness in Portugal: Integrating Community Engagement and Risk ManagementDocument9 pagesEnhancing Forest Fires Preparedness in Portugal: Integrating Community Engagement and Risk Managementputri auliaNo ratings yet
- PDF document-AF8B778E2177-1Document4 pagesPDF document-AF8B778E2177-1Ngoc KimNo ratings yet
- Summer Training Report ON 33/11 KV Sub Station: Duration 09 July 2018 To 02 Sept. 2018Document69 pagesSummer Training Report ON 33/11 KV Sub Station: Duration 09 July 2018 To 02 Sept. 2018Hemanshu DurejaNo ratings yet
- Access Token Stealing On WindowsDocument11 pagesAccess Token Stealing On Windows@4e4enNo ratings yet