You might also like
- Cognitive Development in Anemic Infants of Different PrakritiFrom EverandCognitive Development in Anemic Infants of Different PrakritiNo ratings yet
- CHC374065Document17 pagesCHC374065Antwi EmmanuelNo ratings yet
- Influence of Obesity On Foot Loading Characteristics in Gait For Children Aged 1 To 12 YearsDocument12 pagesInfluence of Obesity On Foot Loading Characteristics in Gait For Children Aged 1 To 12 Yearstania martinezNo ratings yet
- Maciałczyk-Paprocka Et Al. - 2017 - Prevalence of Incorrect Body Posture in Children ADocument10 pagesMaciałczyk-Paprocka Et Al. - 2017 - Prevalence of Incorrect Body Posture in Children ArootNo ratings yet
- Genu Valgum and Flat Feet in Children With Healthy.15Document7 pagesGenu Valgum and Flat Feet in Children With Healthy.15saarita lozano piedraNo ratings yet
- Association Between A Comprehensive Movement Assesment and MetabolicallyDocument9 pagesAssociation Between A Comprehensive Movement Assesment and MetabolicallyzunigasanNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument8 pagesInternational Journal of Pediatric OtorhinolaryngologyCaro JaramilloNo ratings yet
- Growth After Adenotonsillectomy For Obstructive Sleep Apnea: An RCTDocument10 pagesGrowth After Adenotonsillectomy For Obstructive Sleep Apnea: An RCTCalvin AffendyNo ratings yet
- HTTPS-::WWW Nature Com:articles:pr2003504Document8 pagesHTTPS-::WWW Nature Com:articles:pr2003504LucyFloresNo ratings yet
- ObaraGolebiowska Et AlDocument10 pagesObaraGolebiowska Et Al-Katarzyna -No ratings yet
- El Índice de Postura Del Pie, Prueba de Estocada Del Tobillo La Escala de Beighton y La Evaluación de Las Extremidades Inferiores Puntaje en Niños Sanos: Un Estudio de ConfiabilidadDocument5 pagesEl Índice de Postura Del Pie, Prueba de Estocada Del Tobillo La Escala de Beighton y La Evaluación de Las Extremidades Inferiores Puntaje en Niños Sanos: Un Estudio de ConfiabilidadNairda Teresa Arredondo CruzNo ratings yet
- Original Contribution Increased Prevalence of Sleep-Disordered Breathing in AdultsDocument12 pagesOriginal Contribution Increased Prevalence of Sleep-Disordered Breathing in AdultsAsti Sauna MentariNo ratings yet
- Validity and Reliability of The International FItness Scale (IFIS)Document23 pagesValidity and Reliability of The International FItness Scale (IFIS)Jam Ali PakistanNo ratings yet
- Effects of Resistance Training in Children and Adolescents A Meta-AnalysisDocument14 pagesEffects of Resistance Training in Children and Adolescents A Meta-AnalysisDenilson CostaNo ratings yet
- 10.1515 - Ijamh 2020 0169Document8 pages10.1515 - Ijamh 2020 0169Muh SutraNo ratings yet
- Bolger 2019Document13 pagesBolger 2019NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Voss Et Al. 2011 Exercise Brain and Cognition Across The Life SpanDocument10 pagesVoss Et Al. 2011 Exercise Brain and Cognition Across The Life SpanHenriqueNo ratings yet
- 2013-Haugen-Valores Normativos Sit and ReachDocument7 pages2013-Haugen-Valores Normativos Sit and ReachChuleNo ratings yet
- Growth After AdenotonsillectomyDocument10 pagesGrowth After AdenotonsillectomyfriscahalimNo ratings yet
- 17 Eman EtalDocument8 pages17 Eman EtaleditorijmrhsNo ratings yet
- Promoting Physical Activity and Fitness: Supporting Individuals with Childhood-Onset DisabilitiesFrom EverandPromoting Physical Activity and Fitness: Supporting Individuals with Childhood-Onset DisabilitiesDésirée B MaltaisNo ratings yet
- Unhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansDocument7 pagesUnhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansJason DenostaNo ratings yet
- Hen 206 13Document8 pagesHen 206 13Alneo LesagNo ratings yet
- Antrhropometry Measurement To Determine Nutritional Status Among Cerebral PalsyDocument6 pagesAntrhropometry Measurement To Determine Nutritional Status Among Cerebral PalsyutariNo ratings yet
- Content ServerDocument9 pagesContent ServerKennie RamirezNo ratings yet
- Phys Ther 2012 Opheim 279 88Document12 pagesPhys Ther 2012 Opheim 279 88Anang FajarNo ratings yet
- Paediatric PhysiologyDocument378 pagesPaediatric PhysiologyVivi Perez Zumbado100% (2)
- IJMRHS VOl 3 Issue 3 With Cover Page v2Document272 pagesIJMRHS VOl 3 Issue 3 With Cover Page v2Muhammad ZubairNo ratings yet
- Jhse Vol 12 N 1 219-235Document17 pagesJhse Vol 12 N 1 219-235Maybelle E. EraNo ratings yet
- The Effects of a Family Fitness Program on the Physical Activity and Nutrition Behaviors of Third Grade ChildrenDocument11 pagesThe Effects of a Family Fitness Program on the Physical Activity and Nutrition Behaviors of Third Grade ChildrenJones AnkomahNo ratings yet
- Pediatric Physiology 2007Document378 pagesPediatric Physiology 2007Andres Jeria Diaz100% (1)
- Marques - 2017 - Associations Between Self Reported Fitness and Self Rated HealthDocument4 pagesMarques - 2017 - Associations Between Self Reported Fitness and Self Rated Healthricadroval10No ratings yet
- Relationship of Body Fat and Cardiorespiratory Fitness With Cardiovascular Risk in Chinese ChildrenDocument5 pagesRelationship of Body Fat and Cardiorespiratory Fitness With Cardiovascular Risk in Chinese ChildrenArya KusumaNo ratings yet
- 2016 Article 144Document5 pages2016 Article 144Radwa TalaatNo ratings yet
- Pediatrics 2010 Nafiu E306 10 PDFDocument7 pagesPediatrics 2010 Nafiu E306 10 PDFDesty Adjaahh LaahhNo ratings yet
- DOHaD and Birth Cohort ResearchDocument3 pagesDOHaD and Birth Cohort ResearchNguyễn Tiến HồngNo ratings yet
- Obesity and Iron Metabolism LinkDocument6 pagesObesity and Iron Metabolism LinkAhmed SobhNo ratings yet
- Prenatal and Postnatal Exposure To PFAS and Cardiometabolic - 2021 - EnvironmentDocument11 pagesPrenatal and Postnatal Exposure To PFAS and Cardiometabolic - 2021 - EnvironmentAlexander VassilevNo ratings yet
- 10.1542@Peds.2012-0764.PDF Junal Nutrition 1Document9 pages10.1542@Peds.2012-0764.PDF Junal Nutrition 1bobkevinNo ratings yet
- The Female Athlete Triad: A Clinical GuideFrom EverandThe Female Athlete Triad: A Clinical GuideCatherine M. GordonNo ratings yet
- Original Article: Vikawati, NE Sarosa, H Rosdiana, IDocument6 pagesOriginal Article: Vikawati, NE Sarosa, H Rosdiana, IAriyantoNo ratings yet
- E782 FullDocument10 pagesE782 FullDân NguyễnNo ratings yet
- 2019 Article AbstractsFromThe5thInternation PDFDocument41 pages2019 Article AbstractsFromThe5thInternation PDFStephano NgangiNo ratings yet
- Objective Parallel-Forms Reliability Assessment of 3 Dimension Real Time Body Posture Screening TestsDocument9 pagesObjective Parallel-Forms Reliability Assessment of 3 Dimension Real Time Body Posture Screening TestsMonikaNo ratings yet
- BACIL, Eliane Denise, Et Al Physical Activity and Biological Maturation A Systematic Review. Rev Paul Pediatr. v.33, n.1, P. 114-121, 2015.Document8 pagesBACIL, Eliane Denise, Et Al Physical Activity and Biological Maturation A Systematic Review. Rev Paul Pediatr. v.33, n.1, P. 114-121, 2015.Carlos Augusto FaccoNo ratings yet
- Mishra2017 PDFDocument9 pagesMishra2017 PDFJuan Jesus Gomez AlarconNo ratings yet
- Oddy WH, 2018 PDFDocument12 pagesOddy WH, 2018 PDFAnibal LeNo ratings yet
- Swallowing Kinematic Differences Across Frozen, Mixed, and Ultrathin Liquid Boluses in Healthy Adults: Age, Sex, and Normal VariabilityDocument16 pagesSwallowing Kinematic Differences Across Frozen, Mixed, and Ultrathin Liquid Boluses in Healthy Adults: Age, Sex, and Normal Variabilitymackay00917No ratings yet
- Dyw 236Document12 pagesDyw 236Fatamorgana AbdullahNo ratings yet
- Ortega 2011 Reference ValuesDocument11 pagesOrtega 2011 Reference ValuesCarys RobertsNo ratings yet
- Boreham, C., & Riddoch, C. (2001) - The Physical Activity, Fitness and Health ofDocument17 pagesBoreham, C., & Riddoch, C. (2001) - The Physical Activity, Fitness and Health ofAnonymous TLQn9SoRRbNo ratings yet
- Journal of A Ffective Disorders: Research PaperDocument7 pagesJournal of A Ffective Disorders: Research PaperangelavillateavilaNo ratings yet
- 26 Audh Ampun Aduh AmpunDocument3 pages26 Audh Ampun Aduh Ampundel AjjahNo ratings yet
- Health-Related Quality of Life of Children and Adolescents With CKD Stages 4-5 and Their CaregiversDocument12 pagesHealth-Related Quality of Life of Children and Adolescents With CKD Stages 4-5 and Their CaregiversariNo ratings yet
- Prospective Longitudinal Assessmentof Linear Growthand Adult Heightin Female Adolescents With Anorexia Nervosa 2020Document11 pagesProspective Longitudinal Assessmentof Linear Growthand Adult Heightin Female Adolescents With Anorexia Nervosa 2020tekstschrijverdanielleNo ratings yet
- 56-29-PBDocument129 pages56-29-PBMarianneNo ratings yet
- Occupation, Physical Fitness and Adiposity Markers Among Security Guards and Students of Delhi UniversityDocument8 pagesOccupation, Physical Fitness and Adiposity Markers Among Security Guards and Students of Delhi UniversityPradeepNo ratings yet
- Teaching Exercise to Children: A Complete Guide to Theory and PracticeFrom EverandTeaching Exercise to Children: A Complete Guide to Theory and PracticeRating: 5 out of 5 stars5/5 (1)
- ploegstra2016, crescimento x hipertensão pulmonar em pediatriaDocument10 pagesploegstra2016, crescimento x hipertensão pulmonar em pediatrialaerciomoreiradearaujomoreiraNo ratings yet
- Journal of Vocational Health StudiesDocument6 pagesJournal of Vocational Health StudiesDyah SafitriNo ratings yet
- Marcha Normal e Patológica 1Document34 pagesMarcha Normal e Patológica 1Anonymous YePlm1vHz7No ratings yet
- Six Minute Walk Test (6MWT) Instructions: Set UpDocument2 pagesSix Minute Walk Test (6MWT) Instructions: Set UpnikhilNo ratings yet
- Article in Press: Brachial Plexus Birth Palsy: Management During The First Year of LifeDocument8 pagesArticle in Press: Brachial Plexus Birth Palsy: Management During The First Year of LifeDyah SafitriNo ratings yet
- A Review of The Literature On Evidence-Based Practice in PhysicalDocument10 pagesA Review of The Literature On Evidence-Based Practice in PhysicalDyah SafitriNo ratings yet
- 6 Minute Walk Test ATS GuidelinesDocument7 pages6 Minute Walk Test ATS GuidelinescpradheepNo ratings yet
- Bone Healing Induced by ESWTDocument4 pagesBone Healing Induced by ESWTDyah SafitriNo ratings yet
- Accepted ManuscriptDocument18 pagesAccepted ManuscriptDyah SafitriNo ratings yet
- Birth Brachial Plexus Palsy UpdateDocument8 pagesBirth Brachial Plexus Palsy UpdateDyah SafitriNo ratings yet
- Estimation of The Metabolic Equivalent (Met) of An Exercise Protocol Based On Indirect CalorimetryDocument5 pagesEstimation of The Metabolic Equivalent (Met) of An Exercise Protocol Based On Indirect CalorimetryDyah SafitriNo ratings yet
- Pengumuman Hasil Akhir Seleksi Administrasi CPNS Kemenperin 2021Document532 pagesPengumuman Hasil Akhir Seleksi Administrasi CPNS Kemenperin 2021Dyah Safitri100% (2)
- Dynamic Lung Function Testing ExplainedDocument8 pagesDynamic Lung Function Testing ExplainedHafis HerdimanNo ratings yet
- Chest PT in Icu 1996@609.full PDFDocument17 pagesChest PT in Icu 1996@609.full PDFDyah SafitriNo ratings yet
- 6 Minute Walk Test ATS GuidelinesDocument7 pages6 Minute Walk Test ATS GuidelinescpradheepNo ratings yet
- Who TRMDocument250 pagesWho TRMDaniel Giraldo Toro100% (1)
- Nice Cap SciDocument46 pagesNice Cap SciDyah SafitriNo ratings yet
- Asjsm 06 23206Document6 pagesAsjsm 06 23206Dyah SafitriNo ratings yet
- Aerobic Endurance Training Improves Soccer PerformanceDocument7 pagesAerobic Endurance Training Improves Soccer PerformanceFauzi Al-Kaylani100% (1)
- Cerebral White Matter Damage in The Preterm Infant: Pathophysiology and Risk FactorsDocument13 pagesCerebral White Matter Damage in The Preterm Infant: Pathophysiology and Risk FactorsDyah SafitriNo ratings yet
- 1887Document13 pages1887Dyah SafitriNo ratings yet
- GX30R 100RDocument53 pagesGX30R 100RSergio Garcia100% (1)
- Installation Instructions: Mico Basic 8.6Document2 pagesInstallation Instructions: Mico Basic 8.6Servizio TecnicoNo ratings yet
- Inspection, Test, Marking and RecordsDocument10 pagesInspection, Test, Marking and RecordssuryaNo ratings yet
- PLF-76T Service ManualDocument40 pagesPLF-76T Service Manualapi-3711045100% (1)
- Test 48Document9 pagesTest 48Thị VyNo ratings yet
- Led ComponentsDocument226 pagesLed Componentselcomsrl100% (1)
- Unit 1Document36 pagesUnit 1MonishNo ratings yet
- Comprehensive Elevator ManualDocument23 pagesComprehensive Elevator ManualIlham fitriansyahNo ratings yet
- Quantum Engine Series: Ower AtingsDocument2 pagesQuantum Engine Series: Ower AtingsAlbertoNo ratings yet
- Budget of Lesson Science 9Document14 pagesBudget of Lesson Science 9Hezl Valerie ArzadonNo ratings yet
- محطات الطاقةDocument22 pagesمحطات الطاقةJoe LewisNo ratings yet
- rt8205b Datasheet-06Document28 pagesrt8205b Datasheet-06André Hipnotista100% (1)
- MPU 2201 Online HGNotes - 1 ACADEMIC ESSAYDocument19 pagesMPU 2201 Online HGNotes - 1 ACADEMIC ESSAYtharaaNo ratings yet
- Corrosion RingsDocument1 pageCorrosion RingsRichard More LeonNo ratings yet
- The Oil Kings Cooper en 15522 - PDFDocument5 pagesThe Oil Kings Cooper en 15522 - PDFNan EatonNo ratings yet
- FAI Services Overview SHORTDocument58 pagesFAI Services Overview SHORTMariela CarrilloNo ratings yet
- Transformer REFDocument4 pagesTransformer REFs_banerjeeNo ratings yet
- Solex Adj ProcedureDocument6 pagesSolex Adj Procedureprivate 2No ratings yet
- Kinetic and Potential Energy PracticeDocument1 pageKinetic and Potential Energy Practicealchemist2000No ratings yet
- Final Directory Handbook For ADIPEC 2023Document54 pagesFinal Directory Handbook For ADIPEC 2023Zharif ZainiNo ratings yet
- Fundamix Brochure EN WebDocument9 pagesFundamix Brochure EN Webjgjb4csrj7No ratings yet
- General Principles of Freeze Drying (The Lyophilization Process)Document9 pagesGeneral Principles of Freeze Drying (The Lyophilization Process)Shefali PawarNo ratings yet
- Volkswagen 2.0L TDI Common Rail Engine Service TrainingDocument90 pagesVolkswagen 2.0L TDI Common Rail Engine Service TrainingАлла Харютина100% (1)
- KPSC/ KSEB/ SSC Electrical Score Academy: Questions: 75Document9 pagesKPSC/ KSEB/ SSC Electrical Score Academy: Questions: 75sreevasanthNo ratings yet
- Design and implementation of a solar-powered electric smart benchDocument7 pagesDesign and implementation of a solar-powered electric smart benchAmir KalčoNo ratings yet
- YM80SA Abrasive Belt Polishing Machine-Operation ManualDocument7 pagesYM80SA Abrasive Belt Polishing Machine-Operation ManualAgha Ali KhanNo ratings yet
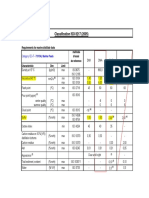
- Classification ISO 8217 (2005)Document5 pagesClassification ISO 8217 (2005)Salah JallaliNo ratings yet
- Equipment & Dimensions: EH4500: Standard Equipment Optional Equipment Eh4500 Ac Wheel MotorDocument2 pagesEquipment & Dimensions: EH4500: Standard Equipment Optional Equipment Eh4500 Ac Wheel MotorAndi Wardiman AnwarNo ratings yet
- Air Motor Torque and Horsepower LabDocument7 pagesAir Motor Torque and Horsepower LabMelody KimNo ratings yet
- GROUP 1 - PetE 3306 - Final Requirement in Engineering EconomicsDocument12 pagesGROUP 1 - PetE 3306 - Final Requirement in Engineering Economicskevin alidoNo ratings yet