You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Simon - Kerblom Abstract PDFDocument1 pageSimon - Kerblom Abstract PDFmau tauNo ratings yet
- Histopathologic Analysis of Appendectomy Specimens: Shrestha R, Ranabhat SR, Tiwari MDocument5 pagesHistopathologic Analysis of Appendectomy Specimens: Shrestha R, Ranabhat SR, Tiwari Mmau tauNo ratings yet
- Blood Supply To BrainDocument29 pagesBlood Supply To BrainwhatervwreasNo ratings yet
- Muhammad Sajid Bin Mohd Rafee 112016389 DR Abraham Sp.UDocument38 pagesMuhammad Sajid Bin Mohd Rafee 112016389 DR Abraham Sp.Umau tauNo ratings yet
- Biomed EthicsDocument12 pagesBiomed EthicsRaz MahariNo ratings yet
- Biomed EthicsDocument115 pagesBiomed Ethicsmau tauNo ratings yet
- Simon Kerblom AbstractDocument1 pageSimon Kerblom Abstractmau tauNo ratings yet
- Respiratory System Assessment in Pediatrics RefDocument34 pagesRespiratory System Assessment in Pediatrics Refmau tauNo ratings yet
- Biomed EthicsDocument12 pagesBiomed EthicsRaz MahariNo ratings yet
- Opportunistic Infection (S2)Document41 pagesOpportunistic Infection (S2)mau tauNo ratings yet
- Opportunistic Infection (S2)Document41 pagesOpportunistic Infection (S2)mau tauNo ratings yet
- Rectum & Anus: DR Darminto Salim Departemen Anatomi FK UkridaDocument14 pagesRectum & Anus: DR Darminto Salim Departemen Anatomi FK Ukridamau tauNo ratings yet
- Lower Limb FracturesDocument124 pagesLower Limb Fracturesmau tau100% (1)
- Abdominal Trauma Agsts 2014Document13 pagesAbdominal Trauma Agsts 2014Florindo Cardoso GomesNo ratings yet
- Opportunistic Infection (S2)Document41 pagesOpportunistic Infection (S2)mau tauNo ratings yet
- Sepsis Kuliah Ukrida Edwin 2014 2 ADocument51 pagesSepsis Kuliah Ukrida Edwin 2014 2 Amau tauNo ratings yet
- Anaphylaxis ReactionDocument27 pagesAnaphylaxis Reactionmau tauNo ratings yet
- Improving Memory Using N-Back TrainingDocument72 pagesImproving Memory Using N-Back Trainingmau tauNo ratings yet
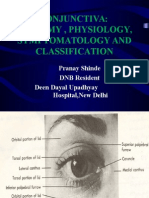
- Conjunctivaanatomyandphysiology 140805084207 Phpapp02Document32 pagesConjunctivaanatomyandphysiology 140805084207 Phpapp02dmurali73No ratings yet
- Jaeggietal Memory2010 ValidityDocument20 pagesJaeggietal Memory2010 Validitymau tauNo ratings yet
- Working Memory, Attention Control and The N-Back TaskDocument8 pagesWorking Memory, Attention Control and The N-Back Taskmau tauNo ratings yet
- Hypertency Emergency Acute PDFDocument12 pagesHypertency Emergency Acute PDFmasdika09No ratings yet
- 2008 Klatzky Etall BRMDocument6 pages2008 Klatzky Etall BRMmau tauNo ratings yet
- ChikungunyaDocument2 pagesChikungunyaRodriguez GuadalupeNo ratings yet
- UntitledDocument6 pagesUntitledmau tauNo ratings yet
- Jurnal LensaDocument2 pagesJurnal Lensamau tauNo ratings yet
- Biophysical Chemistry of The Ageing Eye Lens.: Proquest Document LinkDocument5 pagesBiophysical Chemistry of The Ageing Eye Lens.: Proquest Document Linkmau tauNo ratings yet
- OriginalDocument16 pagesOriginalmau tauNo ratings yet
- Contact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?Document12 pagesContact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?mau tauNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Diabetes Book THAI-ENGDocument100 pagesDiabetes Book THAI-ENGNaharuthai BumrungratanayosNo ratings yet
- Treatment & Management of DiabetesDocument9 pagesTreatment & Management of DiabetesakupunadaNo ratings yet
- Diabetes in The ElderlyDocument24 pagesDiabetes in The ElderlyRAJEEVNo ratings yet
- Sindroma MetabolikDocument24 pagesSindroma MetabolikAnissa Aulia AdjaniNo ratings yet
- D7 11 June Paper 2015finDocument12 pagesD7 11 June Paper 2015finnoxolo dwaneNo ratings yet
- Type 2 Diabetes MellitusDocument7 pagesType 2 Diabetes MellitusCadiz Etrama Di RaizelNo ratings yet
- Literature Review On Hypertension and DiabetesDocument8 pagesLiterature Review On Hypertension and Diabetesafmabhxbudpljr100% (1)
- Bwcs Feedback Final September 2023Document56 pagesBwcs Feedback Final September 2023Babloo50% (2)
- Diabetes Mellitus Management During AnaesthesiaDocument8 pagesDiabetes Mellitus Management During AnaesthesiaTabish JavaidNo ratings yet
- Recombinant DNA TechnologyDocument25 pagesRecombinant DNA Technologymithramithun001No ratings yet
- What Is RedTactonDocument11 pagesWhat Is RedTactonPreethi PadmanabhanNo ratings yet
- Review Shukla 2000 BunDocument9 pagesReview Shukla 2000 BunGeorgiana Cozma FrunzăNo ratings yet
- Review of Medicago SativaDocument10 pagesReview of Medicago SativaUmesh GilhotraNo ratings yet
- Mudra Therapy For DiabetesDocument3 pagesMudra Therapy For DiabetesMeera MishraNo ratings yet
- Diabetes in HaitiDocument5 pagesDiabetes in HaitianthonykarabanowNo ratings yet
- Medical Surgical Nursing (Cantuba)Document37 pagesMedical Surgical Nursing (Cantuba)incognito100% (11)
- Case Study - Sweet LifeDocument9 pagesCase Study - Sweet LifeRomeo ReyesNo ratings yet
- Biochemistry QuizDocument47 pagesBiochemistry QuizmallikaNo ratings yet
- Intermittent FastingDocument36 pagesIntermittent FastingImeNo ratings yet
- Type 1 DiabetesDocument624 pagesType 1 DiabetesErick David Bances Garcia100% (2)
- New Microsoft Word DocumentDocument6 pagesNew Microsoft Word Documentragavan86No ratings yet
- Drugs StudyDocument35 pagesDrugs StudyMark CapillanesNo ratings yet
- AMARYL - Glimepirid TabletDocument14 pagesAMARYL - Glimepirid TabletAANISAHNo ratings yet
- Case Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetDocument27 pagesCase Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetJade HemmingsNo ratings yet
- Borge Fagerli Advanced DietDocument13 pagesBorge Fagerli Advanced Dietchris_blair_1No ratings yet
- Psychological and Behavioral Effects of Hyperinsulinism in GoldfishDocument3 pagesPsychological and Behavioral Effects of Hyperinsulinism in GoldfishIvy Aggabao100% (1)
- Insulin Lispro Sanofi Epar Product Information - en PDFDocument63 pagesInsulin Lispro Sanofi Epar Product Information - en PDFAndreea Claudia NegrilaNo ratings yet
- Mock 3R - Verbal - QDocument7 pagesMock 3R - Verbal - QCherry Grace Articulo DabuconNo ratings yet
- BCSJ 79 1645Document20 pagesBCSJ 79 1645lab sopsNo ratings yet
- 2 DMTAC Clinic CaseDocument13 pages2 DMTAC Clinic CaseOoi Ah Guan100% (1)