You might also like
- Medsurge RationaleDocument8 pagesMedsurge RationaleRose Anne AbivaNo ratings yet
- MaternityDocument52 pagesMaternityeliNo ratings yet
- Signs of increased ICP in infant with hydrocephalusDocument1 pageSigns of increased ICP in infant with hydrocephalusjamesNo ratings yet
- Hyperemesis Gravidarum: Bleeding Complications of PregnancyDocument6 pagesHyperemesis Gravidarum: Bleeding Complications of PregnancykirbsNo ratings yet
- Ob Exam Study Guide The Bible 001 49pgsDocument50 pagesOb Exam Study Guide The Bible 001 49pgsVin Lorenzo CampbellNo ratings yet
- NCLEX Study MaterialDocument40 pagesNCLEX Study MaterialChristie GerconNo ratings yet
- Global Nursing Pediatrics. Nclex - RNDocument14 pagesGlobal Nursing Pediatrics. Nclex - RNNANANo ratings yet
- This Study Resource Was: Silvestri: Saunders Comprehensive Review For The NCLEX-PN Examination, 7th EditionDocument4 pagesThis Study Resource Was: Silvestri: Saunders Comprehensive Review For The NCLEX-PN Examination, 7th EditionNeoGellinNo ratings yet
- Nclex RN Sata CompilationDocument10 pagesNclex RN Sata CompilationJanna mae PatriarcaNo ratings yet
- U World ReproductiveDocument5 pagesU World ReproductiveAce LabosNo ratings yet
- GoodDocument21 pagesGoodVanessaMUeller80% (5)
- AtiDocument4 pagesAtirunnermn88% (8)
- Med Surg Proctored Concept GuideDocument4 pagesMed Surg Proctored Concept GuideKiayaraNo ratings yet
- NCLEXDocument1 pageNCLEXfrank87ali100% (1)
- Positioning principles and protocols for common medical conditionsDocument48 pagesPositioning principles and protocols for common medical conditionsShazaNo ratings yet
- New Born Care 1Document12 pagesNew Born Care 1Tsuyoshi BangNo ratings yet
- Quizlet Comp Review W:picsDocument26 pagesQuizlet Comp Review W:picsJennifer Vicioso100% (1)
- Individual Performance Profile PN Mental Health 2011 Form BDocument4 pagesIndividual Performance Profile PN Mental Health 2011 Form BStan TanNo ratings yet
- ReMar Nurse University 2020 (VT) Student WorkbookDocument50 pagesReMar Nurse University 2020 (VT) Student WorkbookAnderson AlfredNo ratings yet
- A-T-I Endocrine NotesDocument3 pagesA-T-I Endocrine NotesKelseyAnnBarnesNo ratings yet
- Ati RN 2016 Proctor PedsDocument6 pagesAti RN 2016 Proctor PedsStan Tan50% (2)
- Newborn Assessment and CareDocument17 pagesNewborn Assessment and CareMatthew Lee100% (1)
- Pharmocology Drug Cards: InnovarDocument33 pagesPharmocology Drug Cards: InnovarfaizaNo ratings yet
- OB Quizlet3 Nursing Care of ChildrenDocument6 pagesOB Quizlet3 Nursing Care of ChildrenDanielle ShullNo ratings yet
- Labor and DeliveryDocument56 pagesLabor and DeliveryeliNo ratings yet
- Ob Ati StudyDocument22 pagesOb Ati Studylpirman0580% (5)
- Task Delegations For NclexDocument3 pagesTask Delegations For Nclexjenn_028No ratings yet
- NCLEX Helpful HintsDocument2 pagesNCLEX Helpful HintsJamie Antonini GrantNo ratings yet
- Parenting Styles: - Dictatorial or AuthoritarianDocument45 pagesParenting Styles: - Dictatorial or AuthoritarianCourseTree LearningNo ratings yet
- Antidote: Calcium Gluconate or Calcium Chloride: Excessively Frequent Uterine Contractions During PregnancyDocument3 pagesAntidote: Calcium Gluconate or Calcium Chloride: Excessively Frequent Uterine Contractions During PregnancyCohort Six100% (1)
- Mental Health RemediationDocument3 pagesMental Health RemediationAlvin L. Rozier100% (2)
- Hurst Review CDC Infection Control ChartDocument44 pagesHurst Review CDC Infection Control ChartTerry Thun100% (2)
- DO NOT Delegate What You Can EATDocument1 pageDO NOT Delegate What You Can EATMerlin JosephNo ratings yet
- VATI Med Surg RemediationDocument2 pagesVATI Med Surg RemediationestberryNo ratings yet
- 5 Types of QuestionsDocument5 pages5 Types of QuestionsQwequ Gong AnanseNo ratings yet
- Asthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The AsthmaDocument27 pagesAsthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The Asthmasimonedarling100% (1)
- Quizlet (2) RRRRRDocument7 pagesQuizlet (2) RRRRRGina GiammalvoNo ratings yet
- Pharm Review For Hesi From JanaDocument8 pagesPharm Review For Hesi From Janacheyenne.black5205100% (1)
- Immunity 1Document6 pagesImmunity 1Tori RolandNo ratings yet
- Peds Exam 1 ReviewDocument19 pagesPeds Exam 1 ReviewMahreen UmatiyaNo ratings yet
- Rounding Rules11!3!11Document1 pageRounding Rules11!3!11Sheldon SloanNo ratings yet
- RN Plan StudyDocument13 pagesRN Plan Studywestlake12100% (1)
- Ob Peds Meds ListDocument15 pagesOb Peds Meds ListVin Lorenzo Campbell100% (1)
- Alcohol Withdrawal and Dementia Safety TeachingDocument2 pagesAlcohol Withdrawal and Dementia Safety TeachingestberryNo ratings yet
- Pediatric HESI Review 2016Document9 pagesPediatric HESI Review 2016Brittany78% (9)
- Pediatric NursingDocument9 pagesPediatric NursingCreighton A. BayonganNo ratings yet
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZDocument5 pagesVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaNo ratings yet
- ATI RN Nursing Care of Children Online Practice 2019 ADocument4 pagesATI RN Nursing Care of Children Online Practice 2019 Aianshirow834No ratings yet
- Exam 3 Review Med SurgDocument18 pagesExam 3 Review Med SurgCarol ReidNo ratings yet
- When Can I Register For The NCLEX-RN Exam?Document3 pagesWhen Can I Register For The NCLEX-RN Exam?mimNo ratings yet
- Kaplan Focus ReviewDocument9 pagesKaplan Focus ReviewSaidel ElizondoNo ratings yet
- Comprehensive Nclex Notes Easy To Read PDFDocument97 pagesComprehensive Nclex Notes Easy To Read PDFKenia GeorgesNo ratings yet
- MedSurgATI1Document97 pagesMedSurgATI1LeelanRamphal100% (1)
- The Nclex-Pn Cram Sheet: General Test Information Normal Lab ValuesDocument2 pagesThe Nclex-Pn Cram Sheet: General Test Information Normal Lab Valuesroboat96No ratings yet
- NCLEX Updates June 2010Document21 pagesNCLEX Updates June 2010erika_datu100% (1)
- FNP Final TestDocument10 pagesFNP Final TestNelson MandelaNo ratings yet
- Nclex-Rn Test Study GuideDocument199 pagesNclex-Rn Test Study GuideSusan BensonNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Soto - Week 4 CNS Depression PsychoticsDocument2 pagesSoto - Week 4 CNS Depression Psychoticskatiana louisNo ratings yet
- Pharm Exam Ii NotesDocument24 pagesPharm Exam Ii Noteskatiana louisNo ratings yet
- Pharm Exam I NotesDocument19 pagesPharm Exam I Noteskatiana louisNo ratings yet
- Soto - Week 4 Sedative HypnoticsDocument2 pagesSoto - Week 4 Sedative Hypnoticskatiana louisNo ratings yet
- Soto - Week 3 Respiratory QuestionsDocument3 pagesSoto - Week 3 Respiratory Questionskatiana louisNo ratings yet
- Soto - Week 3 Respiratory QuestionsDocument3 pagesSoto - Week 3 Respiratory Questionskatiana louisNo ratings yet
- Pharm Final Exam NotesDocument26 pagesPharm Final Exam Noteskatiana louis100% (1)
- Pharm Exam I NotesDocument19 pagesPharm Exam I Noteskatiana louisNo ratings yet
- Soto - Week 3 Respiratory QuestionsDocument3 pagesSoto - Week 3 Respiratory Questionskatiana louisNo ratings yet
- Pharm Exam I NotesDocument19 pagesPharm Exam I Noteskatiana louisNo ratings yet
- Soto - Week 2 Lipid QuestionsDocument3 pagesSoto - Week 2 Lipid Questionskatiana louisNo ratings yet
- Pharm Exam Ii NotesDocument24 pagesPharm Exam Ii Noteskatiana louisNo ratings yet
- Preterm Labor and Birth Risk FactorsDocument21 pagesPreterm Labor and Birth Risk Factorskatiana louis100% (1)
- MCN Board Exam QuestionsDocument14 pagesMCN Board Exam QuestionsStephannie Miranda100% (1)
- Comperhensive Nursing L4Document92 pagesComperhensive Nursing L4Max67% (6)
- Guidelines for Nurses and MidwivesDocument7 pagesGuidelines for Nurses and MidwivessabrinajavellanaNo ratings yet
- Postpartum Infectious DiseaseDocument2 pagesPostpartum Infectious DiseaseIvan YeohNo ratings yet
- Post Partum Assessment NCM 107 Care of Mother Child Adolescent Well Client Rle Skills LabDocument10 pagesPost Partum Assessment NCM 107 Care of Mother Child Adolescent Well Client Rle Skills Labskz19914No ratings yet
- Role and Scope ofDocument18 pagesRole and Scope ofLekshmi Manu88% (33)
- MedScholar MDCN Lesson Timetable. June, 2024Document10 pagesMedScholar MDCN Lesson Timetable. June, 202495bc5fgd7jNo ratings yet
- EMLL SSS MaterialDocument40 pagesEMLL SSS MaterialShin KimmyNo ratings yet
- MotherFirst - Maternity Mental Health Strategy: Building Capacity in SaskatchewanDocument64 pagesMotherFirst - Maternity Mental Health Strategy: Building Capacity in SaskatchewankidSKAN Director100% (1)
- Role of Nurse MidwifeDocument31 pagesRole of Nurse MidwiferekhamolNo ratings yet
- MCN 2 Sas Answers 1 46 NVGBFDDocument62 pagesMCN 2 Sas Answers 1 46 NVGBFDcarina.pldtNo ratings yet
- CodingDocument33 pagesCodinglesunk pipiNo ratings yet
- Ncma217 Lec Week10 ModuleDocument10 pagesNcma217 Lec Week10 ModuleABEGAIL BALLORANNo ratings yet
- Chapter 20 - Postpartum Physiologic ChangesDocument10 pagesChapter 20 - Postpartum Physiologic ChangesJill Hill100% (2)
- C. Ask The Mother To Urinate and Empty Her BladderDocument8 pagesC. Ask The Mother To Urinate and Empty Her BladderCzarina Isabela TuazonNo ratings yet
- Day 10-11 - NCM 109 Lec - High Risk Post PartumDocument41 pagesDay 10-11 - NCM 109 Lec - High Risk Post PartumGrey KnighttNo ratings yet
- RMNCH+A Strategy Presentation: Goals, Challenges and InterventionsDocument65 pagesRMNCH+A Strategy Presentation: Goals, Challenges and InterventionsSachin ParmarNo ratings yet
- Gambang SmoDocument4 pagesGambang SmoAlvin ComilaNo ratings yet
- Midwifery Education Module - 3 - Managing Prolonged and Obstructed LabourDocument209 pagesMidwifery Education Module - 3 - Managing Prolonged and Obstructed Labourtsega tilahun100% (1)
- Penurunan Kecemasan Ibu Nifas Menggunakan Totok Wajah Di Fasilitas Pelayanan Persalinan Sumantri, Dewi Susilowati, Dian Kurnia WatiDocument5 pagesPenurunan Kecemasan Ibu Nifas Menggunakan Totok Wajah Di Fasilitas Pelayanan Persalinan Sumantri, Dewi Susilowati, Dian Kurnia WatiadiNo ratings yet
- PMTCT: Ayana Benti (BSC, MSCN,) Wolkite University Department of NursingDocument59 pagesPMTCT: Ayana Benti (BSC, MSCN,) Wolkite University Department of NursingtareNo ratings yet
- Introduction To Home VisitingDocument27 pagesIntroduction To Home VisitingAFTAB H. ABBASINo ratings yet
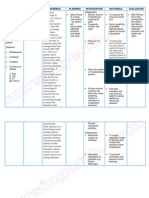
- Nursing Care Plan Postpartum HemorrhageDocument2 pagesNursing Care Plan Postpartum Hemorrhagederic100% (60)
- Adolescent HealthDocument47 pagesAdolescent HealthsushmaNo ratings yet
- DOH-SPMS Form 3 Individual Performance CommitmentDocument4 pagesDOH-SPMS Form 3 Individual Performance CommitmentJohnny Bananao jrNo ratings yet
- Tarifa, Vannesa Joy B. (NU-202) Module 5 Assignment (NCM-109)Document3 pagesTarifa, Vannesa Joy B. (NU-202) Module 5 Assignment (NCM-109)Vannesa TarifaNo ratings yet
- Picot ProposalDocument6 pagesPicot Proposalapi-282602935100% (3)
- Postnatal care planDocument6 pagesPostnatal care planJunaidahMubarakAli100% (1)
- Intrapartum 111: 1. Examine The Woman For Emergency SignsDocument7 pagesIntrapartum 111: 1. Examine The Woman For Emergency SignsJane MartinNo ratings yet
- NGN NCLEX Guide BookDocument94 pagesNGN NCLEX Guide BookMacayMartinezAlexisNo ratings yet