You might also like
- 2005 - Different Approaches Measurement of Hemodynamic by Electrical Impedance Plethysmography MethodDocument2 pages2005 - Different Approaches Measurement of Hemodynamic by Electrical Impedance Plethysmography MethodsuknatsNo ratings yet
- 2000 - Reactions of The Heart Rate and Carotid Artery Pulse Wave Components To The Nitroglycerine UptakeDocument1 page2000 - Reactions of The Heart Rate and Carotid Artery Pulse Wave Components To The Nitroglycerine UptakesuknatsNo ratings yet
- Adc BasicDocument141 pagesAdc BasicthắngNo ratings yet
- Fundamentals of Analog ElectronicsDocument99 pagesFundamentals of Analog Electronicssuknats80% (5)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Noise-Robust Heart Rate Estimation Algorithm From PPG Signal With Low Computacional ComplexityDocument8 pagesNoise-Robust Heart Rate Estimation Algorithm From PPG Signal With Low Computacional ComplexityGiuliano RebuliNo ratings yet
- Matrix T1X PDFDocument20 pagesMatrix T1X PDFAntonio Pérez ÁlvarezNo ratings yet
- Anesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFDocument125 pagesAnesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFKatarina SimicicNo ratings yet
- Rules For EKG StripsDocument5 pagesRules For EKG StripsjessiNo ratings yet
- Daily Lesson Log: PE & HealthDocument5 pagesDaily Lesson Log: PE & HealthJennyNo ratings yet
- Evaluating the Relation Between Maximum Heart Rate and Resting Heart Rate in Three Groups of People Nonathletes الدراسة مهمةathletesDocument4 pagesEvaluating the Relation Between Maximum Heart Rate and Resting Heart Rate in Three Groups of People Nonathletes الدراسة مهمةathletesabdmalek forloulNo ratings yet
- Ecg Holter With Software: User ManualDocument72 pagesEcg Holter With Software: User ManualJhancarlos JuanmacalderonNo ratings yet
- 2016 - Submaximal Exercise Intensity Modulates Acute Post-Exercise Heart Rate VariabilityDocument10 pages2016 - Submaximal Exercise Intensity Modulates Acute Post-Exercise Heart Rate VariabilityVeronica JanethNo ratings yet
- Exercise Physiology Lab ReportDocument14 pagesExercise Physiology Lab ReportRomit Poddar0% (1)
- DiagramDocument7 pagesDiagramEjay Paul C. ColumnasNo ratings yet
- Science of Exercise - Final Course AssignmentDocument2 pagesScience of Exercise - Final Course Assignmentnoxlon75% (4)
- Regression NotesDocument23 pagesRegression Noteslupethe3No ratings yet
- Wujishi Breathing ExerciseDocument167 pagesWujishi Breathing ExerciseRyan Ryan100% (3)
- An Evaluation of The Applicability of The Tripartite Constructs To Social Anxiety in Adolescents Emily R. AndersonDocument14 pagesAn Evaluation of The Applicability of The Tripartite Constructs To Social Anxiety in Adolescents Emily R. AndersonTripartite-ModelNo ratings yet
- 5.3 Importance of High-Speed Fault Clearing: Ieee STD 80-2000 Ieee Guide For SafetyDocument2 pages5.3 Importance of High-Speed Fault Clearing: Ieee STD 80-2000 Ieee Guide For SafetyAnkit AgarwalNo ratings yet
- Daphnia Write UpDocument3 pagesDaphnia Write UpASDFGHJKL9571% (7)
- SympatheticDocument10 pagesSympatheticSharneeshriyaNo ratings yet
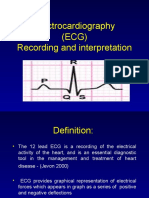
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- Seminars in Fetal & Neonatal Medicine: Michael P. NageotteDocument5 pagesSeminars in Fetal & Neonatal Medicine: Michael P. NageotteElena ZepedaNo ratings yet
- Worksheet Ap06Document7 pagesWorksheet Ap06liawijayaNo ratings yet
- Anesthesia of BearsDocument6 pagesAnesthesia of BearsRafael HaddadNo ratings yet
- Matrix t4 t5x Owners ManualDocument15 pagesMatrix t4 t5x Owners ManualJose MustienesNo ratings yet
- Conditioning ExerciseDocument16 pagesConditioning ExercisenaeemullahNo ratings yet
- Fdar NCPDocument16 pagesFdar NCPshiNo ratings yet
- BME354 - ECG I, Biopotential Amplfier Advaitha Anne TA: Demi ShenDocument5 pagesBME354 - ECG I, Biopotential Amplfier Advaitha Anne TA: Demi ShenanneNo ratings yet
- P eDocument96 pagesP eJoseph KasingNo ratings yet
- NRPDocument8 pagesNRPaeyousefNo ratings yet
- Biofeedback LibroDocument16 pagesBiofeedback LibroLuis A Gil PantojaNo ratings yet
- Polar RS300X User Manual EnglishDocument46 pagesPolar RS300X User Manual EnglishKamil KamalNo ratings yet
- Cardiac Output and Its Control: Made By: Dr. Zara BatoolDocument18 pagesCardiac Output and Its Control: Made By: Dr. Zara BatoolZuhaib AhmedNo ratings yet