You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
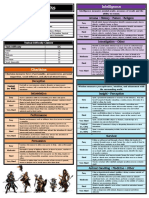
- DM Screen - PortraitDocument5 pagesDM Screen - PortraitEsteban BernsNo ratings yet
- R351Document3 pagesR351ArunBaskarNo ratings yet
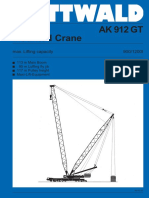
- Pluma Reforzada AK-912 PDFDocument19 pagesPluma Reforzada AK-912 PDFJorge Luis Aguilar AlvaNo ratings yet
- Avatar: The Last Airbender/Legend of Korra Tabletop RPGDocument5 pagesAvatar: The Last Airbender/Legend of Korra Tabletop RPGXavier100% (1)
- Pott'S Disease?Document19 pagesPott'S Disease?Syarif MaulanaNo ratings yet
- PE AnatSpineDocument5 pagesPE AnatSpineEeqNo ratings yet
- DR - Kriengchai - HemostasisDocument35 pagesDR - Kriengchai - HemostasisSyarif MaulanaNo ratings yet
- Human Anatomy & Physiology: Spinal Cord, Spinal Nerves and Somatic ReflexesDocument41 pagesHuman Anatomy & Physiology: Spinal Cord, Spinal Nerves and Somatic ReflexesSyarif MaulanaNo ratings yet
- The Spine EngDocument30 pagesThe Spine EngSyarif MaulanaNo ratings yet
- 8Document10 pages8Syarif MaulanaNo ratings yet
- Prolene Hernia System: David C. Treen, JRDocument14 pagesProlene Hernia System: David C. Treen, JRSyarif MaulanaNo ratings yet
- MIMO Frequency Sampling Filters For Mimo Frequency Sampling Filters For Modelling of MIMO System Applications Modelling ofDocument24 pagesMIMO Frequency Sampling Filters For Mimo Frequency Sampling Filters For Modelling of MIMO System Applications Modelling ofSyarif MaulanaNo ratings yet
- Data RsDocument11 pagesData RsmaryamNo ratings yet
- PMH ResultsDocument1 pagePMH ResultsSyarif MaulanaNo ratings yet
- Jurnal Medical and Health, Volume 2, No., 2015:: Keywords: Lipstick, Individual Identification, GenderDocument10 pagesJurnal Medical and Health, Volume 2, No., 2015:: Keywords: Lipstick, Individual Identification, GenderSyarif MaulanaNo ratings yet
- AbstractDocument1 pageAbstractSyarif MaulanaNo ratings yet
- A Comparative Study of The Efficacy and Safety of Mirtazapine Versus Amitriptyline in The Treatment of Major DepressionDocument6 pagesA Comparative Study of The Efficacy and Safety of Mirtazapine Versus Amitriptyline in The Treatment of Major DepressionSyarif MaulanaNo ratings yet
- Nutritional Knowledge Attitudes and Junk Food Consumption HabitsDocument3 pagesNutritional Knowledge Attitudes and Junk Food Consumption HabitsSyarif MaulanaNo ratings yet
- Laryngeal Mask Airway and Its Variants: Dr. Jayashree SoodDocument6 pagesLaryngeal Mask Airway and Its Variants: Dr. Jayashree SoodParama DinaNo ratings yet
- Rheumatoid Arthritis, Depressive Symptoms and Inflammation: Letter To The Editor 186Document1 pageRheumatoid Arthritis, Depressive Symptoms and Inflammation: Letter To The Editor 186Syarif MaulanaNo ratings yet
- History of LMA New - BackgroundDocument28 pagesHistory of LMA New - BackgroundSyarif MaulanaNo ratings yet
- History of LMA New - BackgroundDocument28 pagesHistory of LMA New - BackgroundSyarif MaulanaNo ratings yet
- International Anesthesiology Clinics 2000 CampoDocument17 pagesInternational Anesthesiology Clinics 2000 CampoSyarif MaulanaNo ratings yet
- Airway ManagementDocument66 pagesAirway ManagementMohamed NorNo ratings yet
- LMA Talk Kelvin 2010 AGDocument26 pagesLMA Talk Kelvin 2010 AGGbotemi AlaladeNo ratings yet
- Laryngeal Mask Airway Update 2005Document11 pagesLaryngeal Mask Airway Update 2005Syarif MaulanaNo ratings yet
- International Anesthesiology Clinics 2000 CampoDocument17 pagesInternational Anesthesiology Clinics 2000 CampoSyarif MaulanaNo ratings yet
- Laryn Mask AirwayDocument6 pagesLaryn Mask AirwaySyarif MaulanaNo ratings yet
- PMH ResultsDocument1 pagePMH ResultsSyarif MaulanaNo ratings yet
- 1 05 209pendekatan Diagnosis LimfadenopatiDocument6 pages1 05 209pendekatan Diagnosis LimfadenopatiTinto Nonii LoveNo ratings yet
- PMH ResultsDocument1 pagePMH ResultsSyarif MaulanaNo ratings yet
- Diseases 05 00017Document6 pagesDiseases 05 00017Syarif MaulanaNo ratings yet
- Hypertension: Detection, Evaluation and Non-Pharmacologic InterventionDocument55 pagesHypertension: Detection, Evaluation and Non-Pharmacologic InterventionSyarif MaulanaNo ratings yet
- Nina - GminDocument3 pagesNina - GminColinNo ratings yet
- Metodo Yamaha 1 A 8Document8 pagesMetodo Yamaha 1 A 8Mariano GonzálezNo ratings yet
- KuihaDocument3 pagesKuihaĞěə ŤğAb TsiNo ratings yet
- Steering Column Tilt PDFDocument26 pagesSteering Column Tilt PDFDaniel OlariNo ratings yet
- MK11 - Fatality ListDocument1 pageMK11 - Fatality ListJobasces MarinNo ratings yet
- Pathology of Peripheral Nerve and Skeletal Muscle - DADocument46 pagesPathology of Peripheral Nerve and Skeletal Muscle - DASinta Dewi AdityaniNo ratings yet
- MR MeeseeksDocument5 pagesMR MeeseeksAndreea RanettiNo ratings yet
- Pharmacies List: Comprehensive Plus Network - Healthcare InsuranceDocument23 pagesPharmacies List: Comprehensive Plus Network - Healthcare InsuranceshajahanputhusseriNo ratings yet
- Samantha BDocument1 pageSamantha BJoshua QuintalNo ratings yet
- Food Chain Magnate Holistic Summary 3.0Document2 pagesFood Chain Magnate Holistic Summary 3.0joviy50654No ratings yet
- Gelatinous Cube - GURPS RepositoryDocument1 pageGelatinous Cube - GURPS Repositorysupreme_bangirasNo ratings yet
- Lean Mass UpDocument3 pagesLean Mass Upmikasaluffy9No ratings yet
- JCB Workmax 800D (US) Mar 2011Document12 pagesJCB Workmax 800D (US) Mar 2011JCB North America0% (1)
- Club Id Nume Club JudetDocument27 pagesClub Id Nume Club JudetMircea VasileNo ratings yet
- Buku Program Pameran SeniDocument4 pagesBuku Program Pameran SeniFatin FaridahNo ratings yet
- CRC - DORRA QuotationDocument7 pagesCRC - DORRA QuotationMEGAWATT CONTRACTING AND ELECTRICITY COMPANYNo ratings yet
- Mapeh 8 Physical Education 3rd Quarter ScrabbleDocument46 pagesMapeh 8 Physical Education 3rd Quarter Scrabblearjay san juanNo ratings yet
- Actea SpicataDocument4 pagesActea SpicataRaveendra MungaraNo ratings yet
- Catalogo Juegos ps3 1Document12 pagesCatalogo Juegos ps3 1Pocho Juan CruzNo ratings yet
- The Red Warrior Path (MAY-JUL 13)Document20 pagesThe Red Warrior Path (MAY-JUL 13)Lamont RisnerNo ratings yet
- Phase ShiftDocument1 pagePhase ShiftdaniNo ratings yet
- Blood Bowl 2020 Roster Tourney: DonateDocument12 pagesBlood Bowl 2020 Roster Tourney: DonateAlejandro LópezNo ratings yet
- Fifa 19 Xboxone AnzDocument29 pagesFifa 19 Xboxone AnzMuhammad NasrullahNo ratings yet
- BB BB BB BB BB BBDocument8 pagesBB BB BB BB BB BBYuri CiabattiNo ratings yet
- Freedive Earth - Freediving Hypoxia and Approaches To SafetyDocument5 pagesFreedive Earth - Freediving Hypoxia and Approaches To SafetyAryaNo ratings yet
- Universidad Tecnologica de Honduras: Please Remember These Rules When Answering The ExercisesDocument4 pagesUniversidad Tecnologica de Honduras: Please Remember These Rules When Answering The ExercisesJoselin HernandezNo ratings yet