You might also like
- Epilepsi PDFDocument11 pagesEpilepsi PDFJonathan SinartaNo ratings yet
- Komplikasi Dan Prognosis Demam TifoidDocument6 pagesKomplikasi Dan Prognosis Demam TifoidPundi Pandan Putri PinantiNo ratings yet
- DR Atitya-Epilepsi ILAE PDFDocument25 pagesDR Atitya-Epilepsi ILAE PDFRayvan StudioTVNo ratings yet
- Neuritis VestibularisDocument2 pagesNeuritis VestibularisMahesa Kurnianti PutriNo ratings yet
- Demam Ruam: Della Rizki Anggilia 18105Document40 pagesDemam Ruam: Della Rizki Anggilia 18105Della Rizki AnggiliaNo ratings yet
- Cerebral Toxoplasmosis: Diagnosis & ManagementDocument32 pagesCerebral Toxoplasmosis: Diagnosis & ManagementShinta DianNo ratings yet
- Help CfponsetiDocument32 pagesHelp CfponsetiShAi_MyStERiOuSNo ratings yet
- Definisi-Klasifikasi EpilepsiDocument40 pagesDefinisi-Klasifikasi Epilepsianita tri hastuti100% (1)
- Bab I Pendahuluan 1.1 Latar BelakangDocument19 pagesBab I Pendahuluan 1.1 Latar BelakangcikaNo ratings yet
- Laporan Kasus - Buta KortikalDocument31 pagesLaporan Kasus - Buta KortikalwadejackNo ratings yet
- Laporan Kasus Status EpileptikusDocument29 pagesLaporan Kasus Status EpileptikusPuji Yunisyah RahayuNo ratings yet
- MeningoencephalitisDocument58 pagesMeningoencephalitisShillea Olimpia Melyta100% (1)
- Struma Nodusa: Pembimbing: Dr. Rizapahlevi., M.Si., SP.BDocument45 pagesStruma Nodusa: Pembimbing: Dr. Rizapahlevi., M.Si., SP.BAndre Pradnyana100% (1)
- Referat Sudden Death - ForensikDocument44 pagesReferat Sudden Death - ForensikMuhamad PascadhNo ratings yet
- TonsilofaringitisDocument1 pageTonsilofaringitisFadhli Rajif TangkeNo ratings yet
- Ventikular Septal Defect FixDocument18 pagesVentikular Septal Defect FixPutri Sari DewiNo ratings yet
- OphthalmoplegiaDocument5 pagesOphthalmoplegiaPatricia Feliani SitohangNo ratings yet
- SACROILIITISDocument13 pagesSACROILIITISRiana KhairaniNo ratings yet
- Preskas NEFROLITIASISDocument24 pagesPreskas NEFROLITIASISaribfarrasNo ratings yet
- Tonsillitis Diphteri: Literature ReadingDocument28 pagesTonsillitis Diphteri: Literature ReadingFebryantiPBundaayabariq100% (1)
- Dr. Kiki Mohammad Iqbal, SPS: Departemen Neurologi FK Usu / Rsup H. Adam Malik MedanDocument35 pagesDr. Kiki Mohammad Iqbal, SPS: Departemen Neurologi FK Usu / Rsup H. Adam Malik MedangracedumaNo ratings yet
- BPPV TRDocument22 pagesBPPV TRTriaNo ratings yet
- KKD NeuroDocument22 pagesKKD NeuroFerdyNo ratings yet
- Optokinetic Nystagmus TestDocument3 pagesOptokinetic Nystagmus TestRegina CaeciliaNo ratings yet
- Pathfast PresepsinDocument6 pagesPathfast PresepsinWulan Ervinna SimanjuntakNo ratings yet
- Blok-22-Meningitis-Tuberkulosis Fakhrurrozi PratamaDocument16 pagesBlok-22-Meningitis-Tuberkulosis Fakhrurrozi PratamaFakhrurrozi PratamaNo ratings yet
- n378.008 Iris Website Staging of CKD PDFDocument8 pagesn378.008 Iris Website Staging of CKD PDFrutebeufNo ratings yet
- 5W FeverDocument14 pages5W FeverYork GarcíaNo ratings yet
- Congenital GlaucomaDocument27 pagesCongenital Glaucomaanon_373532435No ratings yet
- Referat Mata KeratititsDocument28 pagesReferat Mata KeratititsjantyNo ratings yet
- Hernia Nukleus PulposusDocument36 pagesHernia Nukleus PulposusMuhammad Abdul RahmanNo ratings yet
- Japanese EncephalitisDocument14 pagesJapanese EncephalitisMuhammad Rafli AkbarNo ratings yet
- Case AnakDocument28 pagesCase AnakAmorrita Puspita RatuNo ratings yet
- Referat Motion SicknessDocument26 pagesReferat Motion SicknesspututiaNo ratings yet
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- MeningitisDocument20 pagesMeningitisAmalia Tri UtamiNo ratings yet
- Diagnosis Banding Covid 19Document8 pagesDiagnosis Banding Covid 19shinshinNo ratings yet
- Diagnosis Dan Tatalaksana "TOMCAT" / Dermatitis Paederus: Dr. Ian HuangDocument16 pagesDiagnosis Dan Tatalaksana "TOMCAT" / Dermatitis Paederus: Dr. Ian HuangHafiidz Fatich RosihanNo ratings yet
- Dr. Nyoman - Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) .Document41 pagesDr. Nyoman - Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) .hum2No ratings yet
- Neurogenic BladderDocument25 pagesNeurogenic Bladderyouffa hanna elt misykahNo ratings yet
- Case Report Autoimmune EnsephalitisDocument35 pagesCase Report Autoimmune EnsephalitisAfifah Musyirah Yusuf LubisNo ratings yet
- Farmakologi KortikosteroidDocument41 pagesFarmakologi Kortikosteroiddebbyelvira100% (1)
- Reaksi AnafilaksisDocument29 pagesReaksi AnafilaksisoliviafabitaNo ratings yet
- COMA Dan Penurunan KesadaranDocument40 pagesCOMA Dan Penurunan KesadaranAhmad Shafwan NatsirNo ratings yet
- Operasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarDocument10 pagesOperasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarBlack Clover IdNo ratings yet
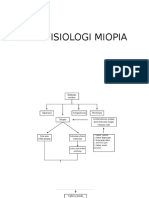
- Patofisiologi MiopiaDocument3 pagesPatofisiologi MiopiaAnonymous g18A6FKiNo ratings yet
- Extrapiramidal Symptom Rating Scale PDFDocument11 pagesExtrapiramidal Symptom Rating Scale PDFsisca satyaNo ratings yet
- Children With Henoch Schonlein Purpura 2.0Document13 pagesChildren With Henoch Schonlein Purpura 2.0soniaNo ratings yet
- Referat NystagmusDocument44 pagesReferat NystagmusNadira Danata100% (1)
- Muntah Pada Anak PDFDocument21 pagesMuntah Pada Anak PDFAndika SiswantaNo ratings yet
- Radioanatomi Jantung Kel 9bDocument42 pagesRadioanatomi Jantung Kel 9bMuhamad KeanuNo ratings yet
- Ohtahara Syndrome: Corticosteroids (Prednisolone or ACTH) Are Occasionally HelpfulDocument2 pagesOhtahara Syndrome: Corticosteroids (Prednisolone or ACTH) Are Occasionally HelpfulidscribddotcomNo ratings yet
- 2017 Tubulointerstitial Nephritis, Diagnosis, Treatment, and MonitoringDocument11 pages2017 Tubulointerstitial Nephritis, Diagnosis, Treatment, and MonitoringbrufenNo ratings yet
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 pagesKolestasis Intrahepatal Vs EkstrahepatalrikarikaNo ratings yet
- DescargaDocument11 pagesDescargaHeath HensleyNo ratings yet
- Status Epileptikus HUT IDI 2017Document31 pagesStatus Epileptikus HUT IDI 2017Aulia Ayu PuspitaNo ratings yet
- Status Epilepticus in Infant and ChildrenDocument85 pagesStatus Epilepticus in Infant and ChildrenAbdullah ShiddiqNo ratings yet
- The EEG of Status Epilepticus: Peter W. KaplanDocument9 pagesThe EEG of Status Epilepticus: Peter W. KaplanNathaly LapoNo ratings yet
- 10.1097@00004691 200409000 00003Document13 pages10.1097@00004691 200409000 00003Ivan MihailovicNo ratings yet
- Medicina: Cognitive Status Epilepticus: Two Case ReportsDocument5 pagesMedicina: Cognitive Status Epilepticus: Two Case ReportsErick SolisNo ratings yet
- Tugas Forensik: Pembimbing: Dr. Baety Adhayati, SP.FDocument18 pagesTugas Forensik: Pembimbing: Dr. Baety Adhayati, SP.FlaurahardiniNo ratings yet
- Timetable For Pediatric TB PDFDocument2 pagesTimetable For Pediatric TB PDFlaurahardiniNo ratings yet
- Questions GynecomastiaDocument4 pagesQuestions GynecomastialaurahardiniNo ratings yet
- CASE REPORT GinekomastiaDocument28 pagesCASE REPORT GinekomastialaurahardiniNo ratings yet
- Weight-For-Age GIRLS: 6 Months To 2 Years (Z-Scores)Document1 pageWeight-For-Age GIRLS: 6 Months To 2 Years (Z-Scores)Malisa LukmanNo ratings yet
- CHT Lfa Girls Z 6 2Document1 pageCHT Lfa Girls Z 6 2Fadhlan ArdhuhaNo ratings yet
- Jurnal Reading IptDocument2 pagesJurnal Reading IptlaurahardiniNo ratings yet
- Referat SE LauraDocument33 pagesReferat SE LauralaurahardiniNo ratings yet
- Chopra3 PPT ch04Document23 pagesChopra3 PPT ch04Rajeev KumarNo ratings yet
- Referat Status EpileptikusDocument19 pagesReferat Status EpileptikuslaurahardiniNo ratings yet
- Laporan Hasil Praktikum Farmakologi Blok Cardiovascular: Kelompok A 2 - 10Document1 pageLaporan Hasil Praktikum Farmakologi Blok Cardiovascular: Kelompok A 2 - 10laurahardiniNo ratings yet
- Wrap Up: Comparison of Hand Hygiene Procedures For RemovingDocument1 pageWrap Up: Comparison of Hand Hygiene Procedures For RemovinglaurahardiniNo ratings yet
- Summary of ECG AbnormalitiesDocument8 pagesSummary of ECG AbnormalitiesChristine Nancy NgNo ratings yet
- Hispanic ObesityDocument25 pagesHispanic Obesityapi-253509573No ratings yet
- ASHA Statement On CASDocument3 pagesASHA Statement On CASAGSpeechLPNo ratings yet
- Abbott TDM - Learning - Guide PDFDocument79 pagesAbbott TDM - Learning - Guide PDFericha apriyantiNo ratings yet
- TatDocument10 pagesTatIqbal Naghma0% (2)
- Miss Pushpaleela Vs State of Karnataka and Others On 17 April, 1998Document3 pagesMiss Pushpaleela Vs State of Karnataka and Others On 17 April, 1998Sayan SanyalNo ratings yet
- Journal of Food Composition and AnalysisDocument11 pagesJournal of Food Composition and AnalysisJessica WeaverNo ratings yet
- SCENAR - From Russia With LoveDocument4 pagesSCENAR - From Russia With LoveTom Askew100% (3)
- Counselling-GATHER ApproachDocument23 pagesCounselling-GATHER ApproachAnilkumar JaraliNo ratings yet
- Heart-Ily Fit 19Document4 pagesHeart-Ily Fit 19api-239426184No ratings yet
- Analysis of Commercial Vitamin C TabletsDocument8 pagesAnalysis of Commercial Vitamin C TabletsYh Po75% (4)
- Beyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDDocument9 pagesBeyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDmakolla007No ratings yet
- Module 2 Personality Traits 3Document6 pagesModule 2 Personality Traits 3Angelica BautistaNo ratings yet
- Peripheral Vascular Disease NursingDocument13 pagesPeripheral Vascular Disease NursingCatlyn Chatpman100% (1)
- Abdominal HerniaDocument3 pagesAbdominal HerniaShenyel Hey'tsmeNo ratings yet
- Blood Warmer ValidationDocument5 pagesBlood Warmer ValidationulgenyNo ratings yet
- Topical Vit C and The SkinDocument4 pagesTopical Vit C and The SkinPaulus AnungNo ratings yet
- Angiotensin II Receptor Blockers-PowerpointDocument16 pagesAngiotensin II Receptor Blockers-PowerpointRoxanne Postrano De VeraNo ratings yet
- The Biopsychosocial Formulation Manual A Guide For Mental Health Professionals PDFDocument178 pagesThe Biopsychosocial Formulation Manual A Guide For Mental Health Professionals PDFLeidy Yiseth Cárdenas100% (4)
- Guía de Diabetes y PsicosisDocument5 pagesGuía de Diabetes y PsicosiskarlunchoNo ratings yet
- Cardio 1stSemSY2014-15 Course SyllabusDocument6 pagesCardio 1stSemSY2014-15 Course SyllabusBeryl Ben MergalNo ratings yet
- Fitzpatricks Dermatology 9th Edition 3124Document1 pageFitzpatricks Dermatology 9th Edition 3124DennisSujayaNo ratings yet
- Sexual AbuseDocument2 pagesSexual AbuseRuth AngelaNo ratings yet
- DR Bachrach Explains Prolo, ThoroughlyDocument14 pagesDR Bachrach Explains Prolo, Thoroughlycindy.laverty5406No ratings yet
- Post TestDocument9 pagesPost TestPradnya Paramitha100% (2)
- Macro Recipe Book Vol 3Document48 pagesMacro Recipe Book Vol 3katia100% (1)
- Ashley's TreatmentDocument3 pagesAshley's TreatmentBrandon M. DennisNo ratings yet
- Serous Fluids AnalysisDocument15 pagesSerous Fluids AnalysisMustafa Khandgawi100% (1)
- Amprahan Obat PustuDocument101 pagesAmprahan Obat Pustuyulinda purwantiNo ratings yet
- 08 - Geriatric Dentistry A ReviewDocument4 pages08 - Geriatric Dentistry A ReviewbkprosthoNo ratings yet