You might also like
- The DIRKS Methodology: A User GuideDocument285 pagesThe DIRKS Methodology: A User GuideJesus Frontera100% (2)
- Employee of The Month.Document2 pagesEmployee of The Month.munyekiNo ratings yet
- Pemicu 4 GIDocument121 pagesPemicu 4 GIFortune De AmorNo ratings yet
- L19 - Pelvic Pain & EndometriosisDocument8 pagesL19 - Pelvic Pain & EndometriosisBrandonRyanF.MosidinNo ratings yet
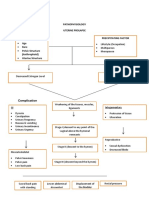
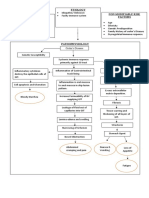
- Pathophysiology HerniaDocument3 pagesPathophysiology HerniaRico Shaun CalapreNo ratings yet
- DPC Cristiane CarboniDocument51 pagesDPC Cristiane CarboniLuis Salazar AscencioNo ratings yet
- Red Flags For Acute Low Back PainDocument5 pagesRed Flags For Acute Low Back PainMaria AgathaNo ratings yet
- Pemicu 4 GITDocument76 pagesPemicu 4 GITtikaNo ratings yet
- Women's HealthDocument8 pagesWomen's HealthkellyjackykjNo ratings yet
- 6.1. Abdominal Pain 讲稿Document5 pages6.1. Abdominal Pain 讲稿mirabel IvanaliNo ratings yet
- Cancer Pain: Departemen Anestesiologi Dan Reanimasi Fakultas Kedokteran USU MedanDocument53 pagesCancer Pain: Departemen Anestesiologi Dan Reanimasi Fakultas Kedokteran USU MedanDONI HERIANTONo ratings yet
- PAIN IN ORTHOPAEDIC DR - ASP EditDocument50 pagesPAIN IN ORTHOPAEDIC DR - ASP EditElisabeth Permatasari SidabutarNo ratings yet
- SURG Abomen CLINICSDocument5 pagesSURG Abomen CLINICSMeg AmoonNo ratings yet
- Acute PancreatitisDocument1 pageAcute PancreatitisJuliane Deniese GregorioNo ratings yet
- AUS 05 History and Physical ExaminationDocument39 pagesAUS 05 History and Physical ExaminationhalayehiahNo ratings yet
- Non Communicable Diseases: Crohn's ArthritisDocument2 pagesNon Communicable Diseases: Crohn's ArthritisJaph Bargayo ChoNo ratings yet
- PATHOPHYSIODocument3 pagesPATHOPHYSIONobby FulgencioNo ratings yet
- Acute Abdominal PainDocument11 pagesAcute Abdominal Painone_2_nv100% (1)
- Clinical Science Session Acute AbdomenDocument28 pagesClinical Science Session Acute AbdomenUlfa Rahmadanti SetiawanNo ratings yet
- Legend: Patient Signs and Symptoms: Manifested by TheDocument2 pagesLegend: Patient Signs and Symptoms: Manifested by TherenelynNo ratings yet
- Structure For History TakingDocument2 pagesStructure For History TakingjonnyjhartNo ratings yet
- Pain ManagementDocument31 pagesPain ManagementNikki Sharmaine VillahermosaNo ratings yet
- Clinical Science Session Acute AbdomenDocument29 pagesClinical Science Session Acute AbdomenNeneng Halimatusa'diahNo ratings yet
- Abdominal PainDocument31 pagesAbdominal PainTarekAlatrozyNo ratings yet
- Pelvic Pain: Dr. Najmah MahmoodDocument58 pagesPelvic Pain: Dr. Najmah Mahmoodشريف محمد حسين شريف يوسفNo ratings yet
- Path o PhysiologyDocument2 pagesPath o PhysiologyshywritesNo ratings yet
- DisorderDocument2 pagesDisorderKrizia TepootNo ratings yet
- WCWMC New Patient PacketDocument18 pagesWCWMC New Patient Packetapi-389559627No ratings yet
- Jsafog 2013 05 147Document7 pagesJsafog 2013 05 147Anna JuniedNo ratings yet
- Differential Abdominal Pain - DR PututDocument28 pagesDifferential Abdominal Pain - DR PututadystiNo ratings yet
- Mari Zita Spa OnDocument57 pagesMari Zita Spa OnMarty BrownNo ratings yet
- Lecture 35 The Acute AbodmenDocument54 pagesLecture 35 The Acute AbodmenMahdi BadarneNo ratings yet
- Chronic Pelvic PainDocument18 pagesChronic Pelvic PainWilliam Alfonso Parada VecinoNo ratings yet
- Bedah II PDFDocument71 pagesBedah II PDFAnggitNo ratings yet
- (GYNE) Dysmenorrhea and Breast Diseases-Dr. Lim (Pingu)Document13 pages(GYNE) Dysmenorrhea and Breast Diseases-Dr. Lim (Pingu)adrian kristopher dela cruzNo ratings yet
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaDocument22 pagesModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'No ratings yet
- Angel Problem 4a GITDocument48 pagesAngel Problem 4a GITMaxend Arselino SilooyNo ratings yet
- Acute Pelvic Pain: HistoryDocument4 pagesAcute Pelvic Pain: HistoryMohamed Al-zichrawyNo ratings yet
- WHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureDocument3 pagesWHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureSreekanth KrishnamurthyNo ratings yet
- Apendisitis: Ronny S, DR, SpotDocument34 pagesApendisitis: Ronny S, DR, SpotLili ManaoNo ratings yet
- Pott's Disease (Pott's Curvature or Angular Kyposis)Document4 pagesPott's Disease (Pott's Curvature or Angular Kyposis)debs0528No ratings yet
- Last Name First Name Middle Name: Medical HistoryDocument2 pagesLast Name First Name Middle Name: Medical HistorySatish R ChilkuryNo ratings yet
- L19 - Pelvic Pain & EndometriosisDocument8 pagesL19 - Pelvic Pain & EndometriosisBrandonRyanF.MosidinNo ratings yet
- The Biology of Chronic Pain - May 2005 (No Pictures)Document40 pagesThe Biology of Chronic Pain - May 2005 (No Pictures)Mike SheatNo ratings yet
- Acute Abdominal Pain in ChildrenDocument82 pagesAcute Abdominal Pain in ChildrensameemNo ratings yet
- Pa Tho Physiology of AchalasiaDocument1 pagePa Tho Physiology of AchalasiaSewyel GarburiNo ratings yet
- Non-Modifiable Risk Factors Etiology Modifiable Risk FactorsDocument13 pagesNon-Modifiable Risk Factors Etiology Modifiable Risk FactorsgabbyNo ratings yet
- INFOGRAPHICDocument1 pageINFOGRAPHICJoyce SumagaysayNo ratings yet
- S-3.dyspepsia + GERD - Dr. AgungDocument58 pagesS-3.dyspepsia + GERD - Dr. AgungFaishalNo ratings yet
- Glossary Medical TermsDocument18 pagesGlossary Medical Termssazmeeta pantaNo ratings yet
- An Approach To The Acute AbdomenDocument6 pagesAn Approach To The Acute AbdomenHardik JeenaNo ratings yet
- Labour Pain and Its Effects v2.0Document23 pagesLabour Pain and Its Effects v2.0Sadhi RashydNo ratings yet
- Inkontinensia Urin: Dr. Adhi Permana, SPPDDocument35 pagesInkontinensia Urin: Dr. Adhi Permana, SPPDTiara KhairinaNo ratings yet
- Chronic Pelvic PainDocument32 pagesChronic Pelvic PainKiyyaa KebedeNo ratings yet
- Low Back Pain: Prof. Dr. Hidayet Sarı Cerrahpaşa Medical School Physical Medicine and Rehabilitation DepartmentDocument87 pagesLow Back Pain: Prof. Dr. Hidayet Sarı Cerrahpaşa Medical School Physical Medicine and Rehabilitation DepartmentAnonymous 1kXBTPvGeuNo ratings yet
- Pa Tho Physiology of Acute AppendicitisDocument1 pagePa Tho Physiology of Acute Appendicitisromeo rivera100% (4)
- Peripheral Neuropathies PathoDocument2 pagesPeripheral Neuropathies PathoSOLEIL LOUISE LACSON MARBASNo ratings yet
- Acupuncture: An Overview of Scientific EvidenceDocument18 pagesAcupuncture: An Overview of Scientific EvidenceIvonne Flores FernándezNo ratings yet
- Group 5 Case 4aDocument83 pagesGroup 5 Case 4aVenny VeronicaNo ratings yet
- Acute AbdomenDocument42 pagesAcute AbdomenErika Agustina KasdjonoNo ratings yet
- Edukasi NyeriDocument52 pagesEdukasi NyeriEko Dakholal FirdausNo ratings yet
- Curing Pelvic Pain: Complete Guide on How to Alleviate and Heal Chronic Pelvic Pain without Going under the KnifeFrom EverandCuring Pelvic Pain: Complete Guide on How to Alleviate and Heal Chronic Pelvic Pain without Going under the KnifeNo ratings yet
- Communication Skill - Time ManagementDocument18 pagesCommunication Skill - Time ManagementChấn NguyễnNo ratings yet
- Monitor 14sepDocument2 pagesMonitor 14sepabhaymvyas1144No ratings yet
- Kallatam of Kallatar (In Tamil Script Tscii Format)Document78 pagesKallatam of Kallatar (In Tamil Script Tscii Format)rprabhuNo ratings yet
- NCP - Impaired Urinary EliminationDocument3 pagesNCP - Impaired Urinary EliminationFretzgine Lou ManuelNo ratings yet
- Gobekli TepeDocument2 pagesGobekli TepeCarl Feagans100% (1)
- Present Tenses ExercisesDocument4 pagesPresent Tenses Exercisesmonkeynotes100% (1)
- Collecting, Analyzing, & Feeding Back DiagnosticDocument12 pagesCollecting, Analyzing, & Feeding Back DiagnosticCaroline Mariae TuquibNo ratings yet
- Dist - Propor.danfoss PVG32Document136 pagesDist - Propor.danfoss PVG32Michal BujaraNo ratings yet
- Sage TutorialDocument115 pagesSage TutorialChhakuli GiriNo ratings yet
- National Insurance Mediclaim Claim FormDocument4 pagesNational Insurance Mediclaim Claim FormIhjaz VarikkodanNo ratings yet
- Makalah Bahasa Inggris TranslateDocument14 pagesMakalah Bahasa Inggris TranslatevikaseptideyaniNo ratings yet
- ES Parent Bulletin Vol#19 2012 May 25Document13 pagesES Parent Bulletin Vol#19 2012 May 25International School ManilaNo ratings yet
- Febrile Neutropenia GuidelineDocument8 pagesFebrile Neutropenia GuidelineAslesa Wangpathi PagehgiriNo ratings yet
- Dynamic Study of Parabolic Cylindrical Shell A Parametric StudyDocument4 pagesDynamic Study of Parabolic Cylindrical Shell A Parametric StudyEditor IJTSRDNo ratings yet
- Sociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadDocument44 pagesSociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadJohn Blackburn100% (20)
- OsciloscopioDocument103 pagesOsciloscopioFredy Alberto Gómez AlcázarNo ratings yet
- Landscape ArchitectureDocument9 pagesLandscape Architecturelisan2053No ratings yet
- Assignment - 1 AcousticsDocument14 pagesAssignment - 1 AcousticsSyeda SumayyaNo ratings yet
- Fce Use of English 1 Teacher S Book PDFDocument2 pagesFce Use of English 1 Teacher S Book PDFOrestis GkaloNo ratings yet
- Legrand Price List-01 ST April-2014Document144 pagesLegrand Price List-01 ST April-2014Umesh SutharNo ratings yet
- Aircraft Wiring Degradation StudyDocument275 pagesAircraft Wiring Degradation Study320338No ratings yet
- FIREBASE Edited PresentationDocument12 pagesFIREBASE Edited PresentationNiraj MirgalNo ratings yet
- DG Oil SpecificationDocument10 pagesDG Oil SpecificationafsalmohmdNo ratings yet
- Diagnosis ListDocument1 pageDiagnosis ListSenyorita KHayeNo ratings yet
- Fertilisation and PregnancyDocument24 pagesFertilisation and PregnancyLopak TikeNo ratings yet
- SL Generator Ultrasunete RincoDocument2 pagesSL Generator Ultrasunete RincoDariaNo ratings yet
- UG ENGLISH Honours PDFDocument59 pagesUG ENGLISH Honours PDFMR.Shantanu SharmaNo ratings yet
- Written Report SampleDocument16 pagesWritten Report Sampleallanposo3No ratings yet