You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Knowing God: Prayer and Fasting 2013Document40 pagesKnowing God: Prayer and Fasting 2013ccforgph100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Black Soldier Fly Larvae ManualDocument14 pagesBlack Soldier Fly Larvae ManualLeonardo Shibata100% (1)
- Soil Loss EstimationDocument77 pagesSoil Loss Estimationmys85No ratings yet
- Financial Plan Checklist: Planning For EmergenciesDocument2 pagesFinancial Plan Checklist: Planning For EmergenciesInsan CornerNo ratings yet
- Automotive ElectronicsDocument44 pagesAutomotive ElectronicsRohit Kumar100% (1)
- Tank Cleaning ConsiderationsDocument1 pageTank Cleaning ConsiderationsAdele PollardNo ratings yet
- Introduction To The Philosophy of The Human PersonDocument17 pagesIntroduction To The Philosophy of The Human Personrovie andes100% (1)
- Boge Screw UsaDocument40 pagesBoge Screw UsaAir Repair, LLC100% (1)
- Social Learning TheoryDocument23 pagesSocial Learning TheoryJacqueline Lacuesta100% (2)
- FLSPfister IB05000 I GBTRWSD0216 MailDocument26 pagesFLSPfister IB05000 I GBTRWSD0216 MailLuis Angel BusturiaNo ratings yet
- MMC 1Document7 pagesMMC 1NikhitaNo ratings yet
- Stat Power PDFDocument40 pagesStat Power PDFNikhitaNo ratings yet
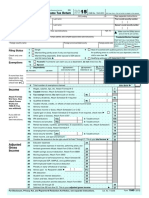
- U.S. Individual Income Tax ReturnDocument2 pagesU.S. Individual Income Tax Returnapi-310622354No ratings yet
- BSC 6432 Syllabus and Schedule Fall 2016-FINAL.081216Document8 pagesBSC 6432 Syllabus and Schedule Fall 2016-FINAL.081216NikhitaNo ratings yet
- Solution Manual For Safety Health and Environmental Concepts For The Process Industry 2nd EditionDocument8 pagesSolution Manual For Safety Health and Environmental Concepts For The Process Industry 2nd EditionRobert Hornback100% (34)
- UntitledDocument77 pagesUntitledVedranL84No ratings yet
- Eye, E.N.T. & Dental AnaesthesiaDocument22 pagesEye, E.N.T. & Dental AnaesthesiawellawalalasithNo ratings yet
- Plant Nematology: A Briefly IntroductionDocument463 pagesPlant Nematology: A Briefly IntroductionRodrigo CarralNo ratings yet
- Step by Step To The Perfect PedicureDocument6 pagesStep by Step To The Perfect PedicurepinkyNo ratings yet
- Edan Sonotrax ManualDocument47 pagesEdan Sonotrax ManualDaniel GalindoNo ratings yet
- Using Casts For ImmobilizationDocument17 pagesUsing Casts For Immobilizationmpmayer2No ratings yet
- An Interview - ExercisesDocument3 pagesAn Interview - ExercisesCarmen GloriaNo ratings yet
- Isoflurane, Sevoflurane and AnestesiDocument124 pagesIsoflurane, Sevoflurane and Anestesizidni fatayanNo ratings yet
- Bemidji Police Department 1-14-13Document19 pagesBemidji Police Department 1-14-13John HagemanNo ratings yet
- ImpetigoDocument31 pagesImpetigoUmmu Insyirah100% (1)
- Homes & Diamonds of Liz TaylorDocument42 pagesHomes & Diamonds of Liz TaylorFridayFunStuffNo ratings yet
- Badhabits 2022Document53 pagesBadhabits 2022Sajad KhaldounNo ratings yet
- 1644 CV Europass Daniel MatosDocument2 pages1644 CV Europass Daniel MatosDaniel MatosNo ratings yet
- MEMBERS AREA IndexDocument13 pagesMEMBERS AREA IndexshahidsarkNo ratings yet
- 631 500seriesvalves PDFDocument2 pages631 500seriesvalves PDFsaiful_tavipNo ratings yet
- Medray Letterhead TemplateDocument5 pagesMedray Letterhead TemplateSteve NjugiNo ratings yet
- Waste Management: Spoilage of LandscapeDocument7 pagesWaste Management: Spoilage of Landscapeshauryasahu2004No ratings yet
- URINALYSISDocument6 pagesURINALYSISmaeNo ratings yet
- NTTM632 Anand Informatica-ETL Lead ResumeDocument8 pagesNTTM632 Anand Informatica-ETL Lead ResumeMohammed JawadNo ratings yet