You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Orthopedic History and Physical Exam GuideDocument28 pagesThe Orthopedic History and Physical Exam GuideAgriya Shresth100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Clinical Chemistry (Lecture) - PrelimsDocument12 pagesClinical Chemistry (Lecture) - Prelimsisprikitik3100% (1)
- Pediatric NursingDocument18 pagesPediatric NursingEinjel Pearl100% (1)
- Blood Transfusion Guide: Types, Storage, Indications & ComplicationsDocument61 pagesBlood Transfusion Guide: Types, Storage, Indications & ComplicationsshikhaNo ratings yet
- Exercise ECGDocument85 pagesExercise ECGSUHER ANUNo ratings yet
- Complete Pediatrics (455-512) 1Document58 pagesComplete Pediatrics (455-512) 1Nimesh Kumara100% (2)
- Sel&Ass&Pae&Lis&Car&1 STDocument198 pagesSel&Ass&Pae&Lis&Car&1 STali tida100% (1)
- eMRCS AnatomyDocument158 pageseMRCS AnatomyNayem Hossain Hemu50% (2)
- Disorders of Potassium, Phosphorus and Magnesium in Critical IllnessDocument6 pagesDisorders of Potassium, Phosphorus and Magnesium in Critical Illnesstaner_soysurenNo ratings yet
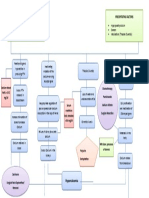
- Concept Map Hypercalcemia FinalDocument1 pageConcept Map Hypercalcemia FinalQueenie Rose Arsenal100% (1)
- ImmunityDocument70 pagesImmunityisprikitik30% (2)
- Sas 17Document3 pagesSas 17Sistine Rose LabajoNo ratings yet
- WHO - Current PartnersDocument2 pagesWHO - Current Partnersisprikitik3No ratings yet
- 8activity Log Journal For MEN and WomenDocument2 pages8activity Log Journal For MEN and Womenisprikitik3No ratings yet
- 6warm Up Conditioning-ExercisesDocument7 pages6warm Up Conditioning-Exercisesisprikitik3No ratings yet
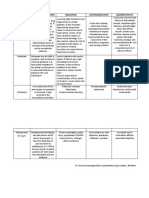
- Drugs Mechanism of Action Indication Contraindication Adverse EffectsDocument2 pagesDrugs Mechanism of Action Indication Contraindication Adverse Effectsisprikitik3No ratings yet
- CD RADIO Upper and Lower ExtDocument12 pagesCD RADIO Upper and Lower Extisprikitik3No ratings yet
- Cyanide Poisoning Written ReportDocument5 pagesCyanide Poisoning Written Reportisprikitik3No ratings yet
- IM Inside (Therapeutic Index Template)Document2 pagesIM Inside (Therapeutic Index Template)isprikitik3No ratings yet
- Evaluation - For External Trainings 06222017Document1 pageEvaluation - For External Trainings 06222017isprikitik3No ratings yet
- Biochemistry 1.6 - ABO Blood Typing and Crossmatching (A1 Group 6)Document68 pagesBiochemistry 1.6 - ABO Blood Typing and Crossmatching (A1 Group 6)isprikitik3No ratings yet
- Ao Final ProgramDocument16 pagesAo Final Programisprikitik3No ratings yet
- Crown Lengthening of ToothDocument4 pagesCrown Lengthening of Toothisprikitik3No ratings yet
- Individual Reflections FormatDocument1 pageIndividual Reflections Formatisprikitik3No ratings yet
- Manuscript Group 2 CPHDocument30 pagesManuscript Group 2 CPHKrisha Mae SalazarNo ratings yet
- Sample HistoryDocument1 pageSample Historyisprikitik3No ratings yet
- God's Creation: Christianity Is An Abrahamic, Monotheistic Religion Based On The Life and OralDocument2 pagesGod's Creation: Christianity Is An Abrahamic, Monotheistic Religion Based On The Life and Oralisprikitik3No ratings yet
- Recommendation LetterDocument1 pageRecommendation Letterisprikitik3No ratings yet
- Request LetterDocument1 pageRequest Letterisprikitik3No ratings yet
- World LitDocument4 pagesWorld Litisprikitik3No ratings yet
- Individual Reflections Format (CPH)Document2 pagesIndividual Reflections Format (CPH)isprikitik3No ratings yet
- Authorization LetterDocument1 pageAuthorization Letterisprikitik3No ratings yet
- Intro To My CologyDocument86 pagesIntro To My Cologyisprikitik3No ratings yet
- World LitDocument4 pagesWorld Litisprikitik3No ratings yet
- Excuse LettersDocument7 pagesExcuse Lettersisprikitik3No ratings yet
- Request LetterDocument1 pageRequest Letterisprikitik3No ratings yet
- MycologyDocument3 pagesMycologyisprikitik3No ratings yet
- MicroscopesDocument6 pagesMicroscopesRenz Mervin RiveraNo ratings yet
- Classification of CarbsDocument3 pagesClassification of Carbsisprikitik3No ratings yet
- Dentist: _____________________________ Assistant: _____________________________ DentistDocument2 pagesDentist: _____________________________ Assistant: _____________________________ DentistregieNo ratings yet
- Acca Cs Syok SepsisDocument1 pageAcca Cs Syok SepsisSamuel KalonkNo ratings yet
- Autoimmune Disorders: By: Kashif Qamar AfridiDocument24 pagesAutoimmune Disorders: By: Kashif Qamar Afridikashmala afzalNo ratings yet
- Hodgkin's DiseaseDocument28 pagesHodgkin's DiseasebikeyNo ratings yet
- C M B G T: Avernous Alformations of The Asal Anglia and HalamusDocument13 pagesC M B G T: Avernous Alformations of The Asal Anglia and HalamusZdravko HeinrichNo ratings yet
- Poster LESDocument6 pagesPoster LESAlejandra LuqueNo ratings yet
- Tatsumi 1997Document9 pagesTatsumi 1997dad dzd adaNo ratings yet
- Cowell and Tyler's Diagnostic Cytology and Hematology of The Dog and Cat (Fifth Edition)Document18 pagesCowell and Tyler's Diagnostic Cytology and Hematology of The Dog and Cat (Fifth Edition)Alexandra AndreeaNo ratings yet
- Anti MalariaDocument28 pagesAnti MalariaselviaNo ratings yet
- The Management of Parkinson's Disease:: Which Treatments To Start and When?Document14 pagesThe Management of Parkinson's Disease:: Which Treatments To Start and When?Andreas StathatosNo ratings yet
- Bio SampleDocument2 pagesBio SamplezalimchuhanNo ratings yet
- Detect Opportunistic MycosesDocument3 pagesDetect Opportunistic MycosesMaryNo ratings yet
- Dopamine Pathways PDFDocument3 pagesDopamine Pathways PDFMuhammad Zul Fahmi AkbarNo ratings yet
- Blood Is Thicker Than WaterDocument4 pagesBlood Is Thicker Than WateraontreochNo ratings yet
- Endocrine System Multiple Choice QuestionsDocument42 pagesEndocrine System Multiple Choice QuestionswanderagroNo ratings yet
- Filariasis Parasite Infection and TransmissionDocument60 pagesFilariasis Parasite Infection and TransmissionDanielle Pecson100% (1)
- GpatDocument21 pagesGpatDeepak Kumar100% (1)
- Behandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Document217 pagesBehandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Ishan ShahNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationAngelica Charisse BuliganNo ratings yet
- Er Alfa Er Beta 2014Document45 pagesEr Alfa Er Beta 2014EN Ka ERNo ratings yet