You might also like
- B. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactDocument4 pagesB. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactJohnpeter EsporlasNo ratings yet
- Amyotrophic Lateral SclerosisDocument3 pagesAmyotrophic Lateral SclerosisJohnpeter EsporlasNo ratings yet
- Parables of Jesus ChristDocument4 pagesParables of Jesus ChristJohnpeter EsporlasNo ratings yet
- Mes 3Document4 pagesMes 3Johnpeter EsporlasNo ratings yet
- Assistive Devices RealDocument3 pagesAssistive Devices RealJohnpeter EsporlasNo ratings yet
- Achalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionDocument10 pagesAchalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionJohnpeter EsporlasNo ratings yet
- Bible FactsDocument28 pagesBible FactsJohnpeter EsporlasNo ratings yet
- Bell's PalsyDocument9 pagesBell's PalsyJohnpeter EsporlasNo ratings yet
- Pediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageDocument3 pagesPediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageJohnpeter EsporlasNo ratings yet
- Tep 11 Reflexes PrintoutDocument2 pagesTep 11 Reflexes PrintoutJohnpeter EsporlasNo ratings yet
- ReviewDocument10 pagesReviewJohnpeter EsporlasNo ratings yet
- Electrotherapy Parameters For Grand PraxDocument3 pagesElectrotherapy Parameters For Grand PraxJohnpeter EsporlasNo ratings yet
- Introduction To PharmacologyDocument6 pagesIntroduction To PharmacologyJohnpeter EsporlasNo ratings yet
- KneeDocument14 pagesKneeJohnpeter Esporlas100% (1)
- Immob Med BackDocument14 pagesImmob Med BackJohnpeter EsporlasNo ratings yet
- TEP 2, Thera Ex 1 and Physiology 2 SyllabusDocument2 pagesTEP 2, Thera Ex 1 and Physiology 2 SyllabusJohnpeter EsporlasNo ratings yet
- Patient Survey: Step 1 - Group Formation and ProfilesDocument6 pagesPatient Survey: Step 1 - Group Formation and ProfilesJohnpeter EsporlasNo ratings yet
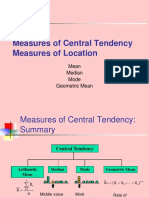
- Central TendencyDocument25 pagesCentral TendencyJohnpeter EsporlasNo ratings yet
- Neuroanatomy Pictures Part 2 - WaxmanDocument6 pagesNeuroanatomy Pictures Part 2 - WaxmanJohnpeter EsporlasNo ratings yet
- Chapter 12Document22 pagesChapter 12John EmmanuelNo ratings yet
- 1st Lecture Sir JomaDocument7 pages1st Lecture Sir JomaJohnpeter EsporlasNo ratings yet
- CBR Topic Outline 2017-2018Document3 pagesCBR Topic Outline 2017-2018Johnpeter EsporlasNo ratings yet
- CVA - Compilation of All BooksDocument4 pagesCVA - Compilation of All BooksJohnpeter EsporlasNo ratings yet
- Atlas of Digestive SystemDocument3 pagesAtlas of Digestive SystemJohnpeter EsporlasNo ratings yet
- Normal Body TemperaturesDocument5 pagesNormal Body TemperaturesJohnpeter EsporlasNo ratings yet
- Anthropometric SDocument3 pagesAnthropometric SJohnpeter EsporlasNo ratings yet
- Down SyndromeDocument2 pagesDown SyndromeJohnpeter EsporlasNo ratings yet
- Cardiovascular RehabilitationDocument5 pagesCardiovascular RehabilitationJohnpeter EsporlasNo ratings yet
- Etiology, Epidemiology & Differential Diagnosis For CADDocument9 pagesEtiology, Epidemiology & Differential Diagnosis For CADJohnpeter EsporlasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- N118 0XYGEN Checklist FinalDocument7 pagesN118 0XYGEN Checklist FinalAmandaNo ratings yet
- Quiz 2Document3 pagesQuiz 2air france bargamentoNo ratings yet
- Stress Management OutlineDocument7 pagesStress Management OutlineJericko Allen Resus100% (1)
- Speech Contest - Stunting in Indonesia2Document2 pagesSpeech Contest - Stunting in Indonesia2Hermawan ChenNo ratings yet
- Example of Health GenogramDocument1 pageExample of Health Genogramapi-322059527No ratings yet
- These Are The Characteristics of The K To 12 Health CurriculumDocument2 pagesThese Are The Characteristics of The K To 12 Health CurriculumKe An U100% (7)
- REGO ET EL TQUK Assessment Syllabus 5-15-2023Document41 pagesREGO ET EL TQUK Assessment Syllabus 5-15-2023Itz Lovaboi ChurchillNo ratings yet
- Swadesh FoundationDocument8 pagesSwadesh FoundationKunal RajNo ratings yet
- REFERENCEDocument2 pagesREFERENCErodolfo opidoNo ratings yet
- Review Related LiteratureDocument3 pagesReview Related LiteraturerdsamsonNo ratings yet
- Reynolds Child Depression Scale ArticleDocument9 pagesReynolds Child Depression Scale ArticleColette MeeNo ratings yet
- Livelihood Sustainabilityof Street Vendors AStudyin Dhaka CityDocument8 pagesLivelihood Sustainabilityof Street Vendors AStudyin Dhaka CityNathaniel PohNo ratings yet
- Nhóm 3 - For MergeDocument5 pagesNhóm 3 - For Mergetrongphap.0203No ratings yet
- Pembukaan Survei Pendampingan Akreditasi Rsu Permata Bunda - GroboganDocument14 pagesPembukaan Survei Pendampingan Akreditasi Rsu Permata Bunda - GroboganAli MuhsonNo ratings yet
- Final - 2022 Nutrition Month PresentationDocument44 pagesFinal - 2022 Nutrition Month PresentationRaynaldo Jr. Del ValleNo ratings yet
- Gianna Graziani Cover LetterDocument1 pageGianna Graziani Cover Letterapi-733890262No ratings yet
- The Concept of Value AdditionDocument5 pagesThe Concept of Value AdditionNura BasmerNo ratings yet
- Benedict James Roldan BermasDocument4 pagesBenedict James Roldan BermasBenedict James BermasNo ratings yet
- Resume - 2022 07 03 095726Document4 pagesResume - 2022 07 03 095726Nessa LarrierNo ratings yet
- Answer No 3-EditedDocument2 pagesAnswer No 3-EditedAlb AklbNo ratings yet
- Hospital Team Match These Following Jobs Below With Their Definition A B ADocument2 pagesHospital Team Match These Following Jobs Below With Their Definition A B AIlhamNo ratings yet
- ElephantiasisDocument21 pagesElephantiasisPutri Anena AyuNo ratings yet
- Breast CA SeminarDocument60 pagesBreast CA SeminarAliyi MuktarNo ratings yet
- Miraculous Self Healing Homoeopathic Principals Therapeutics Materia Medica Ajit Singh Barn.05633 2foreword PrefaceDocument8 pagesMiraculous Self Healing Homoeopathic Principals Therapeutics Materia Medica Ajit Singh Barn.05633 2foreword PrefacemoumonaNo ratings yet
- Medicine - IJGMP - HUMAN IMMUNO DEFFICIENCY - Adetunji Oladeni Adeniji - NigeriaDocument10 pagesMedicine - IJGMP - HUMAN IMMUNO DEFFICIENCY - Adetunji Oladeni Adeniji - Nigeriaiaset123No ratings yet
- Allergo-Immunology Hour: Food AllergyDocument32 pagesAllergo-Immunology Hour: Food AllergyJill PNo ratings yet
- Full Download Health Safety and Nutrition For The Young Child 9th Edition Marotz Test BankDocument26 pagesFull Download Health Safety and Nutrition For The Young Child 9th Edition Marotz Test Bankretainalgrainascjy100% (37)
- BENEFITS and Advantages of Love Moon Anion Sanitary NapkinsDocument3 pagesBENEFITS and Advantages of Love Moon Anion Sanitary NapkinsJeamie Janson De GuzmanNo ratings yet
- English: Quarter 2 - Module 1Document12 pagesEnglish: Quarter 2 - Module 1Raquel FranciscoNo ratings yet
- Insomnia: Ola AyeshDocument31 pagesInsomnia: Ola AyeshSalih TahsinNo ratings yet