You might also like
- Dry Chemestry HistoryDocument6 pagesDry Chemestry HistoryIdali AuralNo ratings yet
- Basic GC ColumnDocument12 pagesBasic GC ColumnSamuel BergollaNo ratings yet
- 1870RespSurgMaskDocument1 page1870RespSurgMasknmmMJKJNo ratings yet
- A61m 16/16 (2006.01) A61m 16/08 (2006.01) A61m 16/00 (2006.01) A61m 16/10 (2006.01) A61m 1/00 (2006.01)Document64 pagesA61m 16/16 (2006.01) A61m 16/08 (2006.01) A61m 16/00 (2006.01) A61m 16/10 (2006.01) A61m 1/00 (2006.01)nmmMJKJNo ratings yet
- TEPZZ Z88Z - A - T: European Patent ApplicationDocument24 pagesTEPZZ Z88Z - A - T: European Patent ApplicationnmmMJKJNo ratings yet
- Introductio NF To Biomedical Equipment Technology: Wiley, 1981 Fll. 75 PP 430Document1 pageIntroductio NF To Biomedical Equipment Technology: Wiley, 1981 Fll. 75 PP 430nmmMJKJNo ratings yet
- Network Decoupling - From Regular To Depthwise Separable ConvolutionsDocument12 pagesNetwork Decoupling - From Regular To Depthwise Separable ConvolutionsArthur M. ColléNo ratings yet
- European Patent Specification: Humidification SystemDocument72 pagesEuropean Patent Specification: Humidification SystemnmmMJKJNo ratings yet
- Is The Deconvolution Layer The Same As A Convolutional LayerDocument7 pagesIs The Deconvolution Layer The Same As A Convolutional LayerabcdefNo ratings yet
- 214 Fractalnet Ultra Deep Neural NDocument11 pages214 Fractalnet Ultra Deep Neural NnmmMJKJNo ratings yet
- A Review Steam Sterilization A Method of SterilizaDocument5 pagesA Review Steam Sterilization A Method of Sterilizadana40018256No ratings yet
- A61M 16/16 (2006.01) F24F 6/00 (2006.01) : Av Ailable)Document59 pagesA61M 16/16 (2006.01) F24F 6/00 (2006.01) : Av Ailable)nmmMJKJNo ratings yet
- Innovative Hand Exoskeleton Design For Extravehicular Activities in SpaceDocument98 pagesInnovative Hand Exoskeleton Design For Extravehicular Activities in SpacenmmMJKJNo ratings yet
- European Patent Application: Respiratory Humidification SystemDocument35 pagesEuropean Patent Application: Respiratory Humidification SystemnmmMJKJNo ratings yet
- Humidification System for Respiratory Therapy DevicesDocument48 pagesHumidification System for Respiratory Therapy DevicesnmmMJKJNo ratings yet
- Interrupter Technique For Assessing Respiratory Resistance: A ReviewDocument6 pagesInterrupter Technique For Assessing Respiratory Resistance: A ReviewnmmMJKJNo ratings yet
- European Patent Application: Respiratory Humidification SystemDocument35 pagesEuropean Patent Application: Respiratory Humidification SystemnmmMJKJNo ratings yet
- Respiratory humidification system controlDocument19 pagesRespiratory humidification system controlnmmMJKJNo ratings yet
- Hamilton Medical HEPA Filter PerformanceDocument2 pagesHamilton Medical HEPA Filter PerformancenmmMJKJNo ratings yet
- Medical Devices Wire and Cable Portfolio: Cables You Trust. Service You DeserveDocument56 pagesMedical Devices Wire and Cable Portfolio: Cables You Trust. Service You DeservenmmMJKJNo ratings yet
- ELISA Technical Manual and Troubleshooting GuideDocument17 pagesELISA Technical Manual and Troubleshooting GuideCHIRANJEEVINo ratings yet
- For Medical Technology: Special CablesDocument20 pagesFor Medical Technology: Special CablesnmmMJKJNo ratings yet
- Uncertainty Related To The Use Of: Relative Retention Times in Pharmaceutical AnalysisDocument7 pagesUncertainty Related To The Use Of: Relative Retention Times in Pharmaceutical AnalysisnmmMJKJNo ratings yet
- Airway Heat & Moisture Exchange Filters (HMEF) : Manufacturer Part # CommentsDocument1 pageAirway Heat & Moisture Exchange Filters (HMEF) : Manufacturer Part # CommentsnmmMJKJNo ratings yet
- Airway Heat & Moisture Exchange Filters (HMEF) : Manufacturer Part # CommentsDocument1 pageAirway Heat & Moisture Exchange Filters (HMEF) : Manufacturer Part # CommentsnmmMJKJNo ratings yet
- Airway Resistance Measured by The Interrupter Technique: Normative Data For 2-10 Year Olds of Three EthnicitiesDocument4 pagesAirway Resistance Measured by The Interrupter Technique: Normative Data For 2-10 Year Olds of Three EthnicitiesnmmMJKJNo ratings yet
- Lung Function PDFDocument15 pagesLung Function PDFAstarinieNo ratings yet
- Standards for BiomaterialsDocument2 pagesStandards for BiomaterialsnmmMJKJNo ratings yet
- Lung Function PDFDocument15 pagesLung Function PDFAstarinieNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Physiological Measurement Handbook (Series in Medical Physics and Biomedical Engineering), 1E (2015) (PDF) (UnitedVRG)Document608 pagesThe Physiological Measurement Handbook (Series in Medical Physics and Biomedical Engineering), 1E (2015) (PDF) (UnitedVRG)Bruna FerreiraNo ratings yet
- ECG BasicsDocument34 pagesECG BasicsBeaCeeNo ratings yet
- Electrocardiografo IVY BIOMEDICAL 7800 (Manual)Document53 pagesElectrocardiografo IVY BIOMEDICAL 7800 (Manual)Kaira Romero VivancoNo ratings yet
- ECG QRS Detection AlgorithmDocument11 pagesECG QRS Detection Algorithmxkurt358792No ratings yet
- Junctional Ectopic Tachycardia in Infants and Children: Ranjit I. Kylat MD - Ricardo A. Samson MDDocument8 pagesJunctional Ectopic Tachycardia in Infants and Children: Ranjit I. Kylat MD - Ricardo A. Samson MDCatherine MorrisNo ratings yet
- U.S. ARMY MEDICAL DEPARTMENT CENTER AND SCHOOL GUIDE TO CARDIAC RHYTHMSDocument40 pagesU.S. ARMY MEDICAL DEPARTMENT CENTER AND SCHOOL GUIDE TO CARDIAC RHYTHMSBatraneluNo ratings yet
- Introduction To It - Ites Industry Unit-1 Part-B: Nagarjuna Public SchoolDocument5 pagesIntroduction To It - Ites Industry Unit-1 Part-B: Nagarjuna Public SchoolPraj JainNo ratings yet
- Indonesia aviation medical regulationsDocument43 pagesIndonesia aviation medical regulationsR SetiawanNo ratings yet
- Sample Review Questions in Medical and Surgical Nursing and Sample Board Exam QuestionsDocument22 pagesSample Review Questions in Medical and Surgical Nursing and Sample Board Exam Questionstinea nigraNo ratings yet
- Heart Rate Detection from BallistocardiogramDocument5 pagesHeart Rate Detection from BallistocardiogramEmilio Cánepa100% (1)
- Spectral Analysis of The ECG SignalDocument2 pagesSpectral Analysis of The ECG SignalCamilo BenitezNo ratings yet
- A Classification and Regression Tree Algorithm For Heart Disease Modeling and PredictionDocument9 pagesA Classification and Regression Tree Algorithm For Heart Disease Modeling and PredictionRavindra MSNo ratings yet
- Nurse Julia educates patient on pacemaker procedureDocument29 pagesNurse Julia educates patient on pacemaker procedureAnnica Lozano100% (1)
- EKG Interpretation NursingDocument14 pagesEKG Interpretation NursingTanya ViarsNo ratings yet
- Prediction of Cardiac Arrhythmia Using Machine LearningDocument11 pagesPrediction of Cardiac Arrhythmia Using Machine LearningIJRASETPublicationsNo ratings yet
- Pediatrics ECG by DR Ali Bel KheirDocument9 pagesPediatrics ECG by DR Ali Bel KheirFerasNo ratings yet
- 12 Lead ECG Mod 1Document31 pages12 Lead ECG Mod 1johnmmenahNo ratings yet
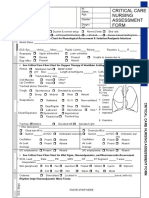
- Idoc - Pub - Critical Care Nursing Assessment FormDocument3 pagesIdoc - Pub - Critical Care Nursing Assessment FormNamra AnsariNo ratings yet
- Operation Manual for Diagnostic Ultrasound System Model SSA-530ADocument90 pagesOperation Manual for Diagnostic Ultrasound System Model SSA-530ANesakkumaren Sivakumaran100% (6)
- EKG Flash Cards PDFDocument9 pagesEKG Flash Cards PDFmattNo ratings yet
- LO 1 Week 3 Caroline AgathaDocument56 pagesLO 1 Week 3 Caroline AgathaCaroline AgathaNo ratings yet
- GE Dash 3000 - Maintenance ProcedureDocument4 pagesGE Dash 3000 - Maintenance ProcedureErickRodríguezCastañedaNo ratings yet
- Nursing Management of CAD and ACSDocument9 pagesNursing Management of CAD and ACSfriendofnurse100% (4)
- 0803616686Document1,132 pages0803616686Nuno Freitas Bastos100% (8)
- Exercise Tolerance TestingDocument15 pagesExercise Tolerance TestingPratyaksha TiwariNo ratings yet
- Pacemaker Sense AmplifiersDocument48 pagesPacemaker Sense AmplifiersArbab Masood AhmadNo ratings yet
- @MedicalBooksStore 2018 Body Sensors and ElectrocardiographyDocument131 pages@MedicalBooksStore 2018 Body Sensors and ElectrocardiographyConstantineSemenchukNo ratings yet
- PLAB Doable Subject Wise PDFDocument1,645 pagesPLAB Doable Subject Wise PDFAbdiNo ratings yet
- UN-M7104 Protocol of ECG ModuleDocument17 pagesUN-M7104 Protocol of ECG ModuleFadjar IftikharNo ratings yet
- Arrhythmia and Conduction Disturbance-AAL-UPH2020Document100 pagesArrhythmia and Conduction Disturbance-AAL-UPH2020Ammar GalihNo ratings yet