You might also like
- Circulatory System QuestionsDocument4 pagesCirculatory System QuestionsJohn Vincent Gonzales50% (2)
- Lung Sounds: An Assessment of The Patient in Respiratory DistressDocument40 pagesLung Sounds: An Assessment of The Patient in Respiratory DistressJoseph Rodney de LeonNo ratings yet
- Lotus Notes Bleeding Letting For ClinicalDocument26 pagesLotus Notes Bleeding Letting For ClinicalMatthieu Decalf100% (2)
- Circulatory and Respiratory ReviewDocument5 pagesCirculatory and Respiratory ReviewNur ShaNo ratings yet
- Patterns of RespirationDocument67 pagesPatterns of Respirationsteven hkNo ratings yet
- Pathology B - Midterm Ratio: Prelim TopicsDocument69 pagesPathology B - Midterm Ratio: Prelim TopicsHuey Manalang JavierNo ratings yet
- (Forensic Pathology Reviews 5) Burkhard Madea, Michael Tsokos, Johanna Preuß (Auth.), Michael Tsokos MD (Eds.) - Forensic Pathology Reviews-Humana Press (2008) PDFDocument289 pages(Forensic Pathology Reviews 5) Burkhard Madea, Michael Tsokos, Johanna Preuß (Auth.), Michael Tsokos MD (Eds.) - Forensic Pathology Reviews-Humana Press (2008) PDFDeo Rafael100% (1)
- Dr. M. Hisham Pediatrics MCQ P.1: RespirationDocument12 pagesDr. M. Hisham Pediatrics MCQ P.1: Respirationعلي. احمد100% (1)
- Thoracic Nerve Anatomy MCQsDocument30 pagesThoracic Nerve Anatomy MCQsKamran Ameer0% (1)
- 4 - Pulmonary PathophysiologyDocument56 pages4 - Pulmonary PathophysiologyReynandriel100% (1)
- ICU TriageDocument27 pagesICU TriageAkmal FahrezzyNo ratings yet
- Cardaic DrugsDocument57 pagesCardaic DrugsJyoti KathwalNo ratings yet
- Circulatory System Multiple Choice QuestionsDocument4 pagesCirculatory System Multiple Choice QuestionsAlee MubeenNo ratings yet
- Medicolegal Aspects of DeathDocument26 pagesMedicolegal Aspects of DeathRonald Alasa-as AtigNo ratings yet
- Scalar Energy PendantDocument12 pagesScalar Energy PendantNicole WeatherleyNo ratings yet
- Upper Respiratory Tract AnatomyDocument61 pagesUpper Respiratory Tract Anatomyيحيى اسماعيل الجميليNo ratings yet
- Ests School of Thoracic SurgeryDocument8 pagesEsts School of Thoracic SurgerybasirNo ratings yet
- 04-CVS - Nader 6 2019+++++++Document14 pages04-CVS - Nader 6 2019+++++++Refan NajiNo ratings yet
- RESIT 2014 PAPER: CERVIX, BREAST, THYROID, HEART DISEASE MCQSDocument3 pagesRESIT 2014 PAPER: CERVIX, BREAST, THYROID, HEART DISEASE MCQSDr-Irfan Habib100% (1)
- COPD and Strep virulence MCQsDocument1 pageCOPD and Strep virulence MCQsSameera DisanayakaNo ratings yet
- Endocrine, Head, and NeckDocument18 pagesEndocrine, Head, and NeckFarhin100% (1)
- 8464 B 1H QP CombinedScienceTrilogy G 16may23 AMDocument32 pages8464 B 1H QP CombinedScienceTrilogy G 16may23 AMMatt A100% (1)
- MCQ More ThoracicDocument8 pagesMCQ More ThoracicWael EssaNo ratings yet
- Science Form 3 Chapter 2Document31 pagesScience Form 3 Chapter 2rosya100% (5)
- Mediastinum Sesat Ix-1Document23 pagesMediastinum Sesat Ix-1kelly christyNo ratings yet
- 06 ChestDocument16 pages06 ChestANAS ALINo ratings yet
- English for Medicine (Part TwoDocument178 pagesEnglish for Medicine (Part TwoShoxruza MusulmonovaNo ratings yet
- Congenital Heart DiseaseDocument45 pagesCongenital Heart DiseaseBrandedlovers OnlineshopNo ratings yet
- CVA Nursing Lesson PlanDocument6 pagesCVA Nursing Lesson Plansimonjosan60% (5)
- BB Sample Exam MCQDocument15 pagesBB Sample Exam MCQbobobo96No ratings yet
- Thoracic Injuries Chapter QuestionsDocument12 pagesThoracic Injuries Chapter QuestionsRifka Anisa0% (1)
- SYLLABUS-2016 CT SurgeryDocument8 pagesSYLLABUS-2016 CT SurgeryGaetano Di GiovanniNo ratings yet
- Survival Rad 15 - Lung HandoutDocument41 pagesSurvival Rad 15 - Lung HandoutLorraineYongNo ratings yet
- 05 Cardiac PDFDocument16 pages05 Cardiac PDFANAS ALINo ratings yet
- Comprehensive Nursing ProcessDocument17 pagesComprehensive Nursing Processm100% (1)
- Thorasic SurgeryDocument124 pagesThorasic SurgeryKoushik Sharma AmancharlaNo ratings yet
- Pulmonary SequestrationDocument15 pagesPulmonary SequestrationEmily EresumaNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- BurnsDocument65 pagesBurnsdhainey100% (1)
- Hypertensive RetinopathyDocument32 pagesHypertensive Retinopathyณัช เกษม100% (7)
- Airway Management Saq 47Document47 pagesAirway Management Saq 47RaMy “MhMd” ElaRabyNo ratings yet
- Biofind and Bioscan WhitepapersDocument15 pagesBiofind and Bioscan WhitepapersCinthia Stephens100% (1)
- Lung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyFrom EverandLung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyPhilip FarrellNo ratings yet
- Perm Issive Hypercapnia: Alex Rogovik,, Ran GoldmanDocument12 pagesPerm Issive Hypercapnia: Alex Rogovik,, Ran GoldmanChristian RíosNo ratings yet
- Final Exam National Board of Examinations JUNE 2020Document2 pagesFinal Exam National Board of Examinations JUNE 2020narasimhahanNo ratings yet
- Tracheobronchial Tree (TBT) : by DR HottorDocument33 pagesTracheobronchial Tree (TBT) : by DR HottorChris ZantiraNo ratings yet
- Preview of "Practice Quiz - Heart"Document2 pagesPreview of "Practice Quiz - Heart"Jose Pagan100% (1)
- X Ray SchemeDocument6 pagesX Ray SchemeIdiAmadouNo ratings yet
- MCQs on skin flaps, burns, trauma and thyroid disordersDocument9 pagesMCQs on skin flaps, burns, trauma and thyroid disordersFarrukh Ali Khan0% (1)
- Pediatric Lung Diseases: Empyema and Lung AbscessDocument39 pagesPediatric Lung Diseases: Empyema and Lung AbscessFaisal MoidunnyNo ratings yet
- Pleural MCQS MedicineDocument17 pagesPleural MCQS MedicineCheryls Raju100% (1)
- RespiratoryDocument57 pagesRespiratoryMuhammad Javed GabaNo ratings yet
- The Management of Acute Respiratory Distress SyndromeDocument48 pagesThe Management of Acute Respiratory Distress SyndromeLauraAlvarezMulettNo ratings yet
- Tracheobronchial TreeDocument51 pagesTracheobronchial TreeravishNo ratings yet
- Cvs MCQDocument52 pagesCvs MCQMiracle For NursesNo ratings yet
- Chest Trauma FinalDocument50 pagesChest Trauma FinalAsim Siddiq VineNo ratings yet
- Scdal 1Document23 pagesScdal 1Cwali MohamedNo ratings yet
- Respiratory System Study GuideDocument13 pagesRespiratory System Study GuidebisnumNo ratings yet
- Acid Base PhysiologyDocument1 pageAcid Base PhysiologyPrabjot SehmiNo ratings yet
- Cardiac AnatomyDocument6 pagesCardiac Anatomysandranamahen2No ratings yet
- FCPS Part1 Recall Ent Sep 2018Document6 pagesFCPS Part1 Recall Ent Sep 2018rizwan afzalNo ratings yet
- How Long Do Partial Thickness Burns Typically Take To Heal?Document49 pagesHow Long Do Partial Thickness Burns Typically Take To Heal?Farah FarahNo ratings yet
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Yu - Git - Emb 2Document56 pagesYu - Git - Emb 2gtaha80No ratings yet
- AtelectasisDocument43 pagesAtelectasismulan557100% (1)
- Cardio-Physiology Exam QuestionsDocument17 pagesCardio-Physiology Exam Questionsjimmy100% (1)
- Benign and Malignant Neoplasia of URTDocument48 pagesBenign and Malignant Neoplasia of URTsahirbuleNo ratings yet
- Anatomy and Physiology of The ThoraxDocument6 pagesAnatomy and Physiology of The ThoraxdocaliNo ratings yet
- Krok 1 - 2014 (Anatomy)Document20 pagesKrok 1 - 2014 (Anatomy)Shameem UabackerNo ratings yet
- Patellar FracturesDocument26 pagesPatellar FracturesDavid VillanuevaNo ratings yet
- Bronchiectasis and Lung Abscess Diagnosis and TreatmentDocument56 pagesBronchiectasis and Lung Abscess Diagnosis and TreatmentMansi GandhiNo ratings yet
- MCQsDocument13 pagesMCQsVinay BhatNo ratings yet
- Medical QuestionsDocument13 pagesMedical QuestionsHannah Lei100% (1)
- RT 220 B C AirwaystudyguideDocument25 pagesRT 220 B C Airwaystudyguiderpebdani0% (2)
- Quiz - Development of Human Cardiovascular SystemDocument7 pagesQuiz - Development of Human Cardiovascular Systemlucky mbaselaNo ratings yet
- Hearts PDFDocument30 pagesHearts PDFLaura RodriguezNo ratings yet
- Summative IV M207Document2 pagesSummative IV M207Thulasi tootsieNo ratings yet
- Renal Patho QuizDocument5 pagesRenal Patho QuizThulasi tootsieNo ratings yet
- Past Year RespiDocument5 pagesPast Year RespiThulasi tootsieNo ratings yet
- Renal Past Year QuestionsDocument3 pagesRenal Past Year QuestionsThulasi tootsieNo ratings yet
- Summative m108Document2 pagesSummative m108Thulasi tootsieNo ratings yet
- Summative m107 Endo, Repro, RenalDocument6 pagesSummative m107 Endo, Repro, RenalThulasi tootsieNo ratings yet
- Pass Year CVSDocument6 pagesPass Year CVSThulasi tootsieNo ratings yet
- MEQ AnswerDocument9 pagesMEQ AnswerThulasi tootsieNo ratings yet
- Ovary PathologyDocument2 pagesOvary PathologyThulasi tootsieNo ratings yet
- RENAL and Reproductive Systems - Q & ADocument13 pagesRENAL and Reproductive Systems - Q & AThulasi tootsieNo ratings yet
- Examination of The Cranial Nerves. Cranial Information. Patient - Patient - CoDocument7 pagesExamination of The Cranial Nerves. Cranial Information. Patient - Patient - CoThulasi tootsieNo ratings yet
- MSK Formative 2012Document13 pagesMSK Formative 2012Thulasi tootsieNo ratings yet
- Mskcns Sum m107Document2 pagesMskcns Sum m107Thulasi tootsieNo ratings yet
- Past Year Me110Document2 pagesPast Year Me110Thulasi tootsieNo ratings yet
- M208 Sum 5Document3 pagesM208 Sum 5Thulasi tootsieNo ratings yet
- Past Year ReproDocument4 pagesPast Year ReproThulasi tootsieNo ratings yet
- Male Genital TractDocument4 pagesMale Genital TractThulasi tootsieNo ratings yet
- Important MechanismDocument2 pagesImportant MechanismThulasi tootsieNo ratings yet
- By WehloongDocument5 pagesBy WehloongThulasi tootsieNo ratings yet
- MEQDocument1 pageMEQThulasi tootsieNo ratings yet
- GI+hemato Past YearDocument9 pagesGI+hemato Past YearThulasi tootsieNo ratings yet
- M109 MSKCNSSummativeDocument5 pagesM109 MSKCNSSummativeThulasi tootsieNo ratings yet
- MalariaDocument1 pageMalariaThulasi tootsieNo ratings yet
- ME110 Summative Sem 5Document17 pagesME110 Summative Sem 5Thulasi tootsieNo ratings yet
- Female Genital TractDocument2 pagesFemale Genital TractThulasi tootsieNo ratings yet
- M208 MSK+CNS Summative (12 Nov 2010)Document11 pagesM208 MSK+CNS Summative (12 Nov 2010)Thulasi tootsieNo ratings yet
- CNS Formative 2012Document17 pagesCNS Formative 2012Ho Yong WaiNo ratings yet
- HematologyDocument39 pagesHematologyThulasi tootsieNo ratings yet
- FS 5 Activity Multiple ChoiceDocument5 pagesFS 5 Activity Multiple ChoiceFritzy Gwen BabaNo ratings yet
- PDF Lecture 9 Benign Soft Tissue TumorsDocument131 pagesPDF Lecture 9 Benign Soft Tissue TumorsMuhammad Rizqi100% (1)
- Fluid DynamicsDocument70 pagesFluid DynamicsH Aries OñaNo ratings yet
- Vital Signs TPRDocument21 pagesVital Signs TPRfloremer guimalanNo ratings yet
- Bio Printing Organs ESL LessonDocument16 pagesBio Printing Organs ESL LessonEnglish OnlineNo ratings yet
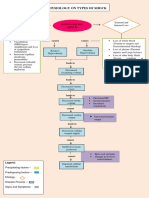
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet
- Exercise 32 Anatomy of Blood Vessels PDFDocument2 pagesExercise 32 Anatomy of Blood Vessels PDFMary0% (1)
- PVS PDF H.Gul PDFDocument34 pagesPVS PDF H.Gul PDFUbaid ullah khanNo ratings yet
- Cardiovascular System ReviewerDocument7 pagesCardiovascular System ReviewerVictoria Ellex TiomicoNo ratings yet
- ARANGUEZ NORTH SECONDARY SCHOO1. IIdocxDocument8 pagesARANGUEZ NORTH SECONDARY SCHOO1. IIdocxDevi RambaranNo ratings yet
- HypertensionDocument5 pagesHypertensionJonathan BreedveldNo ratings yet
- Ebook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFDocument40 pagesEbook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFalexandercampbelldkcnzafgtw100% (10)
- Management of Challenging Cardiopulmonary Bypass SeparationDocument14 pagesManagement of Challenging Cardiopulmonary Bypass SeparationDavid RamirezNo ratings yet
- The Peptide Semax Affect The Expression Genes Related To The Immune and Vascular SystemDocument12 pagesThe Peptide Semax Affect The Expression Genes Related To The Immune and Vascular SystemAlvian VianNo ratings yet
- Animal Physiology Scaffold SheetDocument5 pagesAnimal Physiology Scaffold SheetSuki ChanNo ratings yet