You might also like
- Herbs To Relieve Stress Hoffmann (Keats 1996) PDFDocument108 pagesHerbs To Relieve Stress Hoffmann (Keats 1996) PDFsuperser123465100% (2)
- Upgrade BrainDocument24 pagesUpgrade BrainBranko SlanaNo ratings yet
- Immunology - Chapter 1 OverviewDocument28 pagesImmunology - Chapter 1 OverviewJJHHJHi100% (1)
- Avian Mycoplasmosis Update - 2005Document9 pagesAvian Mycoplasmosis Update - 2005hoodapuneNo ratings yet
- Homeostasis, Stress and Adaptation - Ppt2aDocument154 pagesHomeostasis, Stress and Adaptation - Ppt2aV_RN100% (2)
- Rheumatoid ArthritisDocument33 pagesRheumatoid Arthritisdtpmaharaja100% (1)
- Biology Investigatory Project - Viral DiseasesDocument14 pagesBiology Investigatory Project - Viral DiseasesSamiha Antara81% (127)
- ANOVA - Analysis of Variance (Slides)Document41 pagesANOVA - Analysis of Variance (Slides)medp7060No ratings yet
- Fast Facts: Managing immune-related Adverse Events in Oncology: Early recognition, prompt intervention, effective managementFrom EverandFast Facts: Managing immune-related Adverse Events in Oncology: Early recognition, prompt intervention, effective managementNo ratings yet
- Test Questionairre FormatDocument149 pagesTest Questionairre FormatSantosh Kumar TataNo ratings yet
- R 2006 - Regulatory T Cells, Tumour ImmunityDocument13 pagesR 2006 - Regulatory T Cells, Tumour Immunity1262615286No ratings yet
- CD39 A Promising Target in Oncology PDFDocument9 pagesCD39 A Promising Target in Oncology PDFGeorge Sebastian AntonyNo ratings yet
- Eji 201847659Document7 pagesEji 201847659marjoranovaNo ratings yet
- Avances en Nuevas Estrategias de Vacunas para La Inmunoterapia y Prevención Del Cáncer JAY A. BERZOFSKY 2004Document11 pagesAvances en Nuevas Estrategias de Vacunas para La Inmunoterapia y Prevención Del Cáncer JAY A. BERZOFSKY 2004Ramiro J. Rodriguez GarciaNo ratings yet
- 18 JL 7Document15 pages18 JL 7Irma SihotangNo ratings yet
- Recent Updates On Cancer Immunotherapy: Ming Liu and Fukun GuoDocument10 pagesRecent Updates On Cancer Immunotherapy: Ming Liu and Fukun GuoNicole GarcíaNo ratings yet
- R 2017 - Regulatory T Cells in Cancer ImmunotherapyDocument10 pagesR 2017 - Regulatory T Cells in Cancer Immunotherapy1262615286No ratings yet
- 44 pdl1Document3 pages44 pdl1bawoji1763No ratings yet
- Fonc 08 00086Document14 pagesFonc 08 00086Siska HarapanNo ratings yet
- PD-1 Regulatory T Cells Amplified by PD-1 Blockade Promote Hyperprogression of CancerDocument10 pagesPD-1 Regulatory T Cells Amplified by PD-1 Blockade Promote Hyperprogression of CancerFildza Ahzatil halifahNo ratings yet
- Inmunobiologia CA RenalDocument7 pagesInmunobiologia CA RenalDelia Lucia Escola GomezNo ratings yet
- Artigo ImunologiaDocument13 pagesArtigo ImunologiapaulamonteiromedNo ratings yet
- 10 1016@j TCB 2020 06 003Document10 pages10 1016@j TCB 2020 06 003Maria Aponte RuizNo ratings yet
- Cytotoxic CD8 T Cells in Cancer and Cancer Immunotherapy: Review ArticleDocument9 pagesCytotoxic CD8 T Cells in Cancer and Cancer Immunotherapy: Review ArticleThiKem NguyenNo ratings yet
- Immune Checkpointtargeted Therapy Cancer and Autoimmune Diseases Represent Two Sides of The Same CoinDocument4 pagesImmune Checkpointtargeted Therapy Cancer and Autoimmune Diseases Represent Two Sides of The Same Coinpratiwi eka rahmawatiNo ratings yet
- Tumour Grade Significantly Correlates With Total Dysfunction of Tumour Tissue-Infiltrating Lymphocytes in Renal Cell CarcinomaDocument13 pagesTumour Grade Significantly Correlates With Total Dysfunction of Tumour Tissue-Infiltrating Lymphocytes in Renal Cell Carcinomasara.madkour99No ratings yet
- Targeting T Cell Activation in Immuno-Oncology: S.D. Saibil and P.S. OhashiDocument8 pagesTargeting T Cell Activation in Immuno-Oncology: S.D. Saibil and P.S. OhashiNBME testNo ratings yet
- Quezada 2015. Review Negative Checkpoints Tcells ImmunotherapyDocument30 pagesQuezada 2015. Review Negative Checkpoints Tcells ImmunotherapymcrickboomNo ratings yet
- Cancer Immunosurveillance: AngiogenesisDocument2 pagesCancer Immunosurveillance: AngiogenesisBrenda Bastos LevanoNo ratings yet
- T Cells in Health and DiseaseDocument50 pagesT Cells in Health and Diseaseygilad9139No ratings yet
- HHS Public Access: Cell-Intrinsic Barriers of T Cell-Based ImmunotherapyDocument24 pagesHHS Public Access: Cell-Intrinsic Barriers of T Cell-Based Immunotherapyro111111No ratings yet
- Principles of Cancer Immunotherapy: Authors: Section Editor: Deputy EditorDocument32 pagesPrinciples of Cancer Immunotherapy: Authors: Section Editor: Deputy Editorhochanh199xNo ratings yet
- Gmbar ImunDocument10 pagesGmbar ImunVera FitrianaNo ratings yet
- Cancer Immunology and ImmunotherapyDocument15 pagesCancer Immunology and ImmunotherapyRamona PalalogosNo ratings yet
- Host Defence Mechanisms Against TumorsDocument7 pagesHost Defence Mechanisms Against TumorsHamam AmastrdamNo ratings yet
- Inmunoterapia en Cancer de PulmonDocument7 pagesInmunoterapia en Cancer de PulmonJorge ZegarraNo ratings yet
- +CD103+CD8+ T Cells in Human High-Grade: Transcriptional Activity and Stability of CD39 Endometrial CancerDocument18 pages+CD103+CD8+ T Cells in Human High-Grade: Transcriptional Activity and Stability of CD39 Endometrial CancerSeda KNo ratings yet
- Pone 0093162Document16 pagesPone 0093162Ivonne GutierrezNo ratings yet
- 2.2. Cancer Immunotherapy Co-Stimulatory Agonists and Co-Inhibitory AntagonistsDocument11 pages2.2. Cancer Immunotherapy Co-Stimulatory Agonists and Co-Inhibitory AntagonistsDiego EskinaziNo ratings yet
- CD4 Tregs and Immune Control: Review SeriesDocument9 pagesCD4 Tregs and Immune Control: Review SeriesFelipe Gálvez JirónNo ratings yet
- Lecture 3 Immunology of CancerDocument4 pagesLecture 3 Immunology of CancerAishwarya SinghNo ratings yet
- PharmaceuticsDocument25 pagesPharmaceuticsvera GaborNo ratings yet
- 2021 - CTLA-4 and CD47 On Treg Cells Psolid TumorDocument16 pages2021 - CTLA-4 and CD47 On Treg Cells Psolid Tumor1262615286No ratings yet
- A Game Changer in Cancer TreatmentDocument11 pagesA Game Changer in Cancer TreatmentŞeyma YılmazNo ratings yet
- PosterDocument1 pagePostermomenajib100% (1)
- 157549.2 20220517120354 CoveredDocument15 pages157549.2 20220517120354 CoveredJulián DuránNo ratings yet
- Immune Checkpoint Blockade and CAR-T Cell Therapy in Hematologic MalignanciesDocument20 pagesImmune Checkpoint Blockade and CAR-T Cell Therapy in Hematologic MalignanciesAsfahani LatiefahNo ratings yet
- The Next Decade of Immune Checkpoint Therapy: ReviewDocument21 pagesThe Next Decade of Immune Checkpoint Therapy: ReviewCristina ViaplanaNo ratings yet
- Antigen Presentation in Cancer - Insights Into Tumor Immunogenicity and Immune EvasionDocument15 pagesAntigen Presentation in Cancer - Insights Into Tumor Immunogenicity and Immune EvasionElton De SáNo ratings yet
- Review Article: Viral Modulation of Tlrs and Cytokines and The Related Immunotherapies For Hpv-Associated CancersDocument17 pagesReview Article: Viral Modulation of Tlrs and Cytokines and The Related Immunotherapies For Hpv-Associated CancersmarconijrrNo ratings yet
- Introduction To Immunology and Immunotherapy: Section 1Document13 pagesIntroduction To Immunology and Immunotherapy: Section 1ZairullahMighfazaNo ratings yet
- Impact of Immunotherapy On CD4 T Cell Phenotypes ADocument21 pagesImpact of Immunotherapy On CD4 T Cell Phenotypes APatricia GomesNo ratings yet
- InmunioterapiaDocument8 pagesInmunioterapiaOscar Ivan Sarmiento RamirezNo ratings yet
- Roychoudhuri 2015Document11 pagesRoychoudhuri 2015MaríaFernandaEcheverryNo ratings yet
- Article Journal ClubDocument12 pagesArticle Journal ClubfilymascoloNo ratings yet
- Next Generation of Immune Checkpoint Therapy in Cancer: New Developments and ChallengesDocument20 pagesNext Generation of Immune Checkpoint Therapy in Cancer: New Developments and ChallengesMarcelitaTaliaDuwiriNo ratings yet
- Nri 1936 ArtigoDocument13 pagesNri 1936 ArtigoGlauce L TrevisanNo ratings yet
- Science - Aaa4971 2Document7 pagesScience - Aaa4971 2Alejandro Zuñiga NaterasNo ratings yet
- Anti-CTLA-4 Immunotherapy Does Not Deplete FOXP3þ Regulatory T Cells (Tregs) in Human CancersDocument6 pagesAnti-CTLA-4 Immunotherapy Does Not Deplete FOXP3þ Regulatory T Cells (Tregs) in Human Cancers1262615286No ratings yet
- R 2022 - 代谢Metabolic Profiles &TME of Regulatory TDocument20 pagesR 2022 - 代谢Metabolic Profiles &TME of Regulatory T1262615286No ratings yet
- ImmunoteraphyDocument28 pagesImmunoteraphyMagnusNo ratings yet
- Abstracts For The 27th Annual Scientific Meeting of The Society For Immunotherapy of Cancer (SITC) PDFDocument71 pagesAbstracts For The 27th Annual Scientific Meeting of The Society For Immunotherapy of Cancer (SITC) PDFhigginscribdNo ratings yet
- T Cells With A Single Tumor Antigen Specific T Cell Receptor Can Be Generated in Vitro From Clinically Relevant Stem Cell SourcesDocument13 pagesT Cells With A Single Tumor Antigen Specific T Cell Receptor Can Be Generated in Vitro From Clinically Relevant Stem Cell SourcesGraha NaturNo ratings yet
- Dejaco-Et-Al 06 - (Imbalance of Regulatory T Cells in Human Autoimmune Diseases)Document12 pagesDejaco-Et-Al 06 - (Imbalance of Regulatory T Cells in Human Autoimmune Diseases)Luana DiEmmeNo ratings yet
- Fimmu 13 816005Document14 pagesFimmu 13 816005emmanuel AndemNo ratings yet
- Review Article: The Immune Response To Tumors As A Tool Toward ImmunotherapyDocument12 pagesReview Article: The Immune Response To Tumors As A Tool Toward ImmunotherapyFrontiersNo ratings yet
- Ima y Dasa Reducen MDSCs y Aumentan Respuestas EfectorasDocument12 pagesIma y Dasa Reducen MDSCs y Aumentan Respuestas EfectorasLyanna StarkNo ratings yet
- Innate Lymphoid Cells and Innate-Like T Cells in Cancer - at The Crossroads of Innate and Adaptive ImmunityDocument21 pagesInnate Lymphoid Cells and Innate-Like T Cells in Cancer - at The Crossroads of Innate and Adaptive ImmunityElton De SáNo ratings yet
- Trispecific AntibodyDocument19 pagesTrispecific Antibodys_praviNo ratings yet
- Targeting MYC in Multiple MyelomaDocument12 pagesTargeting MYC in Multiple Myelomamedp7060No ratings yet
- Tumour Heterogeneity and Resistance To Cancer TherapiesDocument14 pagesTumour Heterogeneity and Resistance To Cancer Therapiesmedp7060No ratings yet
- Tumor Heterogeneity and Therapy Resistance - Implications For Future Treatments of Prostate CancerDocument13 pagesTumor Heterogeneity and Therapy Resistance - Implications For Future Treatments of Prostate Cancermedp7060No ratings yet
- Clinical Implications of PTEN Loss in Prostate CancerDocument13 pagesClinical Implications of PTEN Loss in Prostate Cancermedp7060No ratings yet
- Cancer Biomarkers and Targeted TherapiesDocument2 pagesCancer Biomarkers and Targeted Therapiesmedp7060No ratings yet
- Evidence Based Oncology Aug EBO 2017Document44 pagesEvidence Based Oncology Aug EBO 2017medp7060No ratings yet
- Bi123 - The Biology of CancerDocument5 pagesBi123 - The Biology of Cancermedp7060No ratings yet
- Antibody Therapy Against Cancer MM PDFDocument10 pagesAntibody Therapy Against Cancer MM PDFpaNo ratings yet
- Nir 3876Document1 pageNir 3876Sarita RawatNo ratings yet
- Course Syllabus For "BIO404: Cancer Biology"Document5 pagesCourse Syllabus For "BIO404: Cancer Biology"medp7060No ratings yet
- Department of Cancer BiologyDocument2 pagesDepartment of Cancer Biologymedp7060No ratings yet
- Epidermal Growth Factors and CancerDocument2 pagesEpidermal Growth Factors and Cancermedp7060No ratings yet
- The Human Caspase-2 Gene Alternative Promoters, Pre-mRNA Splicing and AUG Usage Direct Isoform-Specific ExpressionDocument12 pagesThe Human Caspase-2 Gene Alternative Promoters, Pre-mRNA Splicing and AUG Usage Direct Isoform-Specific Expressionmedp7060No ratings yet
- Identification of Human Gene Core Promoters in SilicoDocument9 pagesIdentification of Human Gene Core Promoters in Silicomedp7060No ratings yet
- Wind Windy Weather - ExersicesDocument1 pageWind Windy Weather - Exersicesmedp7060No ratings yet
- Better Together Targeted Combination Therapies in Breast CancerDocument9 pagesBetter Together Targeted Combination Therapies in Breast Cancermedp7060No ratings yet
- Trastuzumab Cardiotoxicity in Early-Stage Breast CancerDocument1 pageTrastuzumab Cardiotoxicity in Early-Stage Breast Cancermedp7060No ratings yet
- Targeting HER2 For The Treatment of Breast CancerDocument21 pagesTargeting HER2 For The Treatment of Breast Cancermedp7060No ratings yet
- Breast Cancer and Environment - Breast Cancer ActionDocument5 pagesBreast Cancer and Environment - Breast Cancer Actionmedp7060No ratings yet
- Wind Types of Wind Storm WindsDocument1 pageWind Types of Wind Storm Windsmedp7060No ratings yet
- NatureDocument3 pagesNatureSharad ShresthaNo ratings yet
- Natural Remedies: Causes of Typhoid FeverDocument3 pagesNatural Remedies: Causes of Typhoid FeversakuarNo ratings yet
- Exam Jan 2014Document3 pagesExam Jan 2014Insani Abdi BangsaNo ratings yet
- Immuno GlowDocument11 pagesImmuno GlowNoly ClaveringNo ratings yet
- Autoimmune DiseasesDocument1 pageAutoimmune DiseasesFrances FranciscoNo ratings yet
- The Immune System, Fourth Edition Chapter 4: Antibody Structure and The Generation of B-Cell DiversityDocument23 pagesThe Immune System, Fourth Edition Chapter 4: Antibody Structure and The Generation of B-Cell Diversitylina lopezNo ratings yet
- 2021 Biochem and Genetics Honours ProjectsDocument56 pages2021 Biochem and Genetics Honours ProjectsJuanNo ratings yet
- EUROIMMUN Diagnostic Method For Hypersensitivity in Allergy Reaction FinalDocument52 pagesEUROIMMUN Diagnostic Method For Hypersensitivity in Allergy Reaction Finalgonteng sadyogaNo ratings yet
- Print - Chapter 2. Neurohumoral Regulation of Gastrointestinal FunctionDocument19 pagesPrint - Chapter 2. Neurohumoral Regulation of Gastrointestinal FunctionbelaginaNo ratings yet
- Childrens FBC Reference Ranges PDFDocument1 pageChildrens FBC Reference Ranges PDFWarisatul Imam LubisNo ratings yet
- Bsn3j NCP RosalesDocument6 pagesBsn3j NCP RosalesYvonnie RosalesNo ratings yet
- T Cell From DNA SequencingDocument25 pagesT Cell From DNA SequencingSubhajit DuttaNo ratings yet
- Biology Syllabus For Integrated M.SC Course - Niser Semester 1Document11 pagesBiology Syllabus For Integrated M.SC Course - Niser Semester 1Samyabrata SahaNo ratings yet
- 4-Cell Mediated ImmunityDocument34 pages4-Cell Mediated ImmunityleeminhoangrybirdNo ratings yet
- Theunis, Louise Immunotherapeutics CapstoneDocument4 pagesTheunis, Louise Immunotherapeutics CapstoneLouise TheunisNo ratings yet
- Master of Science in Biochemistry: A Two-Year Full Time Programme (Rules, Regulations and Course Contents)Document40 pagesMaster of Science in Biochemistry: A Two-Year Full Time Programme (Rules, Regulations and Course Contents)Avinash GuptaNo ratings yet
- Development of Safe Juices For Immunocompromised Patients by Irradiation Alone or in Combination With Other TechnologiesDocument245 pagesDevelopment of Safe Juices For Immunocompromised Patients by Irradiation Alone or in Combination With Other Technologies4negeroNo ratings yet
- Cytokines - IntroductionDocument2 pagesCytokines - IntroductionTra gicNo ratings yet
- Chapter 08: Infectious Processes Banasik: Pathophysiology, 6th EditionDocument3 pagesChapter 08: Infectious Processes Banasik: Pathophysiology, 6th EditionAnna ConwayNo ratings yet
- KINE 1020 - Mock Final ExamDocument6 pagesKINE 1020 - Mock Final ExamAlvin MaNo ratings yet
- Crosswords Human HealthDocument1 pageCrosswords Human HealthRiana Ab RahmanNo ratings yet
- Microbios Intestinales en Trastornos Neurocognitivos y de Salud Mental (Halversona y Alagiakrishnan, 2020)Document21 pagesMicrobios Intestinales en Trastornos Neurocognitivos y de Salud Mental (Halversona y Alagiakrishnan, 2020)Centro integral del desarrollo LogrosNo ratings yet
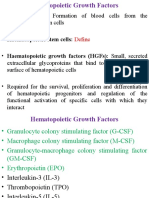
- Hematopoiesis and Growth FactorsDocument17 pagesHematopoiesis and Growth FactorsEmma Joel OtaiNo ratings yet