You might also like
- Ece - 311 LabDocument148 pagesEce - 311 LabSelva RajuNo ratings yet
- Automatic Segmentation of Liver Tumor in CT ImagesDocument6 pagesAutomatic Segmentation of Liver Tumor in CT Imagesmanju.dsatmNo ratings yet
- A Novel Segmentation Approach Combining Region - and Edge-Based Information For Ultrasound ImagesDocument19 pagesA Novel Segmentation Approach Combining Region - and Edge-Based Information For Ultrasound ImagesMia AmaliaNo ratings yet
- Performance Evaluation of TumorDocument12 pagesPerformance Evaluation of TumorAnonymous lVQ83F8mCNo ratings yet
- Idea Proyecto 2Document13 pagesIdea Proyecto 2Marianne GillyNo ratings yet
- Information: A Novel Bio-Inspired Deep Learning Approach For Liver Cancer DiagnosisDocument36 pagesInformation: A Novel Bio-Inspired Deep Learning Approach For Liver Cancer DiagnosiselmannaiNo ratings yet
- 3D Brain Tumor Segmentation in MRI Using Fuzzy Classification, Symmetry Analysis and Spatially Constrained Deformable ModelsDocument17 pages3D Brain Tumor Segmentation in MRI Using Fuzzy Classification, Symmetry Analysis and Spatially Constrained Deformable ModelsGjgjtiuyiuyi RewtesrtertNo ratings yet
- Automated Segmentation and Classi Fication of Hepatocellular Carcinoma Using Fuzzy C-Means and SVMDocument18 pagesAutomated Segmentation and Classi Fication of Hepatocellular Carcinoma Using Fuzzy C-Means and SVMBudi Utami FahnunNo ratings yet
- Bai 2019Document12 pagesBai 2019SINGSTONNo ratings yet
- A Novel Bio-Inspired Deep Learning Approach For LiDocument36 pagesA Novel Bio-Inspired Deep Learning Approach For LiMohamed SalahNo ratings yet
- Segmentation of Prostate Boundaries From Ultrasound Images Using Statistical Shape ModelDocument13 pagesSegmentation of Prostate Boundaries From Ultrasound Images Using Statistical Shape ModelMurat ArarNo ratings yet
- Computers in Biology and Medicine: Vida Harati, Rasoul Khayati, Abdolreza FarzanDocument10 pagesComputers in Biology and Medicine: Vida Harati, Rasoul Khayati, Abdolreza FarzanJosé Ignacio OrlandoNo ratings yet
- Two-Stage Semi-Automatic Organ Segmentation Framework Using Radial Basis Functions and Level SetsDocument10 pagesTwo-Stage Semi-Automatic Organ Segmentation Framework Using Radial Basis Functions and Level Setsvenkeey2No ratings yet
- 05 Ijictv3n9spl PDFDocument6 pages05 Ijictv3n9spl PDFBudi Utami FahnunNo ratings yet
- Kidney Stone Detection Using MatlabDocument22 pagesKidney Stone Detection Using MatlabSania hyder50% (2)
- Applied Sciences: Deep Learning-Based Automatic Segmentation of Mandible and Maxilla in Multi-Center CT ImagesDocument15 pagesApplied Sciences: Deep Learning-Based Automatic Segmentation of Mandible and Maxilla in Multi-Center CT ImagesDyah Dhani MustikariniNo ratings yet
- 2010 Panagiotaki Et Al. Lecture Notes in Computer Science PDFDocument8 pages2010 Panagiotaki Et Al. Lecture Notes in Computer Science PDFAjayaKumarKavalaNo ratings yet
- Vera 2019 J. Phys. Conf. Ser. 1160 012001Document8 pagesVera 2019 J. Phys. Conf. Ser. 1160 012001veramig1396No ratings yet
- Kidney and Tumor Segmentation Using Combined Deep Learning MethodDocument11 pagesKidney and Tumor Segmentation Using Combined Deep Learning MethodegamrNo ratings yet
- A Simple Approach For Relatively Automated Hippocampus Segmentation From Sagittal View of Brain MriDocument8 pagesA Simple Approach For Relatively Automated Hippocampus Segmentation From Sagittal View of Brain MriijbbjournalNo ratings yet
- Effective Brain Segmentation Method Based On MR Physics Image ProcessingDocument14 pagesEffective Brain Segmentation Method Based On MR Physics Image ProcessingAnonymous lt2LFZHNo ratings yet
- Ali 2016Document11 pagesAli 2016Budi Utami FahnunNo ratings yet
- Writing SampleDocument14 pagesWriting SampleYiming JingNo ratings yet
- Symmetry 10 00589 PDFDocument25 pagesSymmetry 10 00589 PDFDewi RahmawatiNo ratings yet
- MODIFIED Synopsis of The Proposed ResearchDocument23 pagesMODIFIED Synopsis of The Proposed ResearchAshokupadhye1955No ratings yet
- Survey Goals Segmentation: Watershed SegmentationDocument3 pagesSurvey Goals Segmentation: Watershed Segmentationjenisha SNo ratings yet
- Effective Kidney Segmentation Using Gradient Based Approach in Abdominal CT ImagesDocument6 pagesEffective Kidney Segmentation Using Gradient Based Approach in Abdominal CT ImagesrajNo ratings yet
- How To Write An AbstractDocument4 pagesHow To Write An AbstractSofiane MouasNo ratings yet
- Texture Based Watershed 3D MI Segmentation Based On Fuzzy Reg Growing Aprch.Document20 pagesTexture Based Watershed 3D MI Segmentation Based On Fuzzy Reg Growing Aprch.rgowda25No ratings yet
- DTI Longitudinal Atlas Construction As An Average of Growth ModelsDocument12 pagesDTI Longitudinal Atlas Construction As An Average of Growth ModelsmarcniethammerNo ratings yet
- Vera 2019 J. Phys. Conf. Ser. 1160 012001Document8 pagesVera 2019 J. Phys. Conf. Ser. 1160 012001veramig1396No ratings yet
- Automatic Measurement of Fetal Femur Length in Ultrasound Images: A Comparison of Random Forest Regression Model and SegnetDocument16 pagesAutomatic Measurement of Fetal Femur Length in Ultrasound Images: A Comparison of Random Forest Regression Model and SegnetSharifahobaid AlrashidiNo ratings yet
- Zhai Et Al 2020 Automatic Orbital Computed Tomography Coordinating Method and Quantitative Error Evaluation Based OnDocument6 pagesZhai Et Al 2020 Automatic Orbital Computed Tomography Coordinating Method and Quantitative Error Evaluation Based OnKevin TandartoNo ratings yet
- Paper 1Document36 pagesPaper 1Ahmed MateenNo ratings yet
- An Automatic Diagnostic System For CT Liver Image ClassificationDocument12 pagesAn Automatic Diagnostic System For CT Liver Image ClassificationShankar GaneshNo ratings yet
- Pancreas Disease Detection and Segmentation Using Abdominal CT ScanDocument9 pagesPancreas Disease Detection and Segmentation Using Abdominal CT ScanIJAR JOURNALNo ratings yet
- Cell Cluster Graph For Prediction of Biochemical Recurrence in Prostate Cancer Patients From Tissue MicroarraysDocument11 pagesCell Cluster Graph For Prediction of Biochemical Recurrence in Prostate Cancer Patients From Tissue MicroarraysFrontiersNo ratings yet
- Detection of Tumour in 3D Brain Image Using Mri Mining TechniquesDocument6 pagesDetection of Tumour in 3D Brain Image Using Mri Mining TechniquesJeevan KishorNo ratings yet
- 20-2007 - Kadoury Et AlDocument12 pages20-2007 - Kadoury Et AlJuan Pablo Romero CamposNo ratings yet
- Temporal Analysis of Mammograms Based On Graph Matching: 1 BackgroundDocument8 pagesTemporal Analysis of Mammograms Based On Graph Matching: 1 BackgroundAnand BalajiNo ratings yet
- Zernike CBM 2011Document10 pagesZernike CBM 2011Jyotsna SinghNo ratings yet
- An Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningDocument7 pagesAn Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningInternational Organization of Scientific Research (IOSR)No ratings yet
- Retina Blood Vessel SegmentationDocument28 pagesRetina Blood Vessel SegmentationRevati WableNo ratings yet
- CT-based Deep Learning Segmentation of Ovarian Cancer and The Stability of The Extracted Radiomics FeaturesDocument12 pagesCT-based Deep Learning Segmentation of Ovarian Cancer and The Stability of The Extracted Radiomics Featuressukeshini jadhavNo ratings yet
- Sensors: Multi-Modality Medical Image Fusion Using Convolutional Neural Network and Contrast PyramidDocument17 pagesSensors: Multi-Modality Medical Image Fusion Using Convolutional Neural Network and Contrast PyramidShrida Prathamesh KalamkarNo ratings yet
- A Statistical Atlas of Prostate Cancer For Optimal Biopsy: Email: Dgshen@cbmv - Jhu.edu, Hristos@rad - Jhu.eduDocument9 pagesA Statistical Atlas of Prostate Cancer For Optimal Biopsy: Email: Dgshen@cbmv - Jhu.edu, Hristos@rad - Jhu.eduJacquelineNo ratings yet
- Soft-Tissues Image Processing: Comparison of Traditional Segmentation Methods With 2D Active Contour MethodsDocument9 pagesSoft-Tissues Image Processing: Comparison of Traditional Segmentation Methods With 2D Active Contour Methodsdiankusuma123No ratings yet
- Radiographic Bone Texture Analysis Using Deep Learning Models For Early Rheumatoid Arthritis DiagnosisDocument15 pagesRadiographic Bone Texture Analysis Using Deep Learning Models For Early Rheumatoid Arthritis DiagnosisRaj PanchalNo ratings yet
- Ijcrt2105065 1Document4 pagesIjcrt2105065 1Sheba ParimalaNo ratings yet
- A Spleen Segmentation Method Based On PCA-ISODocument6 pagesA Spleen Segmentation Method Based On PCA-ISOJanice AbrahamNo ratings yet
- A Survey of Image Processing Techniques For Detection of MassDocument6 pagesA Survey of Image Processing Techniques For Detection of MassInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- MAP-Based Framework For Segmentation of MR Brain Images Based On Visual Appearance and Prior ShapeDocument13 pagesMAP-Based Framework For Segmentation of MR Brain Images Based On Visual Appearance and Prior ShapeNuthangi MaheshNo ratings yet
- A Hybrid Approach For Liver SegmentationDocument10 pagesA Hybrid Approach For Liver SegmentationMarckus BrodyNo ratings yet
- Deep Semantic Segmentation of Kidney and Space-Occupying Lesion Area Based On SCNN and Resnet Models Combined With Sift-Flow AlgorithmDocument12 pagesDeep Semantic Segmentation of Kidney and Space-Occupying Lesion Area Based On SCNN and Resnet Models Combined With Sift-Flow AlgorithmMuhamad Praja DewanataNo ratings yet
- SynSeg Net Synthetic Segmentation Without Target Modality Ground TruthDocument10 pagesSynSeg Net Synthetic Segmentation Without Target Modality Ground TruthKshitij AgarwalNo ratings yet
- Breast Cancer Screening Using Convolutional NeuralDocument13 pagesBreast Cancer Screening Using Convolutional NeuralAkash BSDKNo ratings yet
- Reliability of A Powerpoint Method For Wear Measurement After Total Hip ArthroplastyDocument8 pagesReliability of A Powerpoint Method For Wear Measurement After Total Hip Arthroplastyfahrul muhammadNo ratings yet
- Surface ReConstruction of Dicom Images FinalDocument8 pagesSurface ReConstruction of Dicom Images FinalDavid DivadNo ratings yet
- Literature Survey On Detection of Brain Tumor From MRI ImagesDocument7 pagesLiterature Survey On Detection of Brain Tumor From MRI ImagesInternational Organization of Scientific Research (IOSR)No ratings yet
- Automated Tumor Segmentation in MR Brain Image Using Fuzzy C-Means Clustering and Seeded Region MethodologyDocument7 pagesAutomated Tumor Segmentation in MR Brain Image Using Fuzzy C-Means Clustering and Seeded Region MethodologyIAES IJAINo ratings yet
- High Performance Deformable Image Registration Algorithms for Manycore ProcessorsFrom EverandHigh Performance Deformable Image Registration Algorithms for Manycore ProcessorsNo ratings yet
- University Grants Commission Net Bureau: Syllabus SubjectDocument4 pagesUniversity Grants Commission Net Bureau: Syllabus Subjectmnb11augNo ratings yet
- An AI Assistant For Visually Impaired PersonDocument8 pagesAn AI Assistant For Visually Impaired PersonAnanyaja DebadiptaNo ratings yet
- 802.11 Security - Wired Equivalent Privacy (WEP) : by Shruthi B KrishnanDocument19 pages802.11 Security - Wired Equivalent Privacy (WEP) : by Shruthi B KrishnanAnanyaja DebadiptaNo ratings yet
- Shri Harinama Mahamantra (Hindi)Document75 pagesShri Harinama Mahamantra (Hindi)Mukesh K. AgrawalNo ratings yet
- Gate New Syllabus Computer Science and Information Technology For 2016Document2 pagesGate New Syllabus Computer Science and Information Technology For 2016ersayantanNo ratings yet
- Wireless CommunicationDocument21 pagesWireless Communicationasifmagsi415No ratings yet
- Syllabus FOR M. SC. Computer ScienceDocument31 pagesSyllabus FOR M. SC. Computer ScienceAnanyaja DebadiptaNo ratings yet
- HTML Essentials Cheat Sheet PDFDocument1 pageHTML Essentials Cheat Sheet PDFwilliamNo ratings yet
- Mca 1 Semester Operating System With Lab (MCC - 1.5) Full Marks - 100 (Mid Semester Lab: 20 Marks End Semester: 80 Marks)Document2 pagesMca 1 Semester Operating System With Lab (MCC - 1.5) Full Marks - 100 (Mid Semester Lab: 20 Marks End Semester: 80 Marks)Ananyaja DebadiptaNo ratings yet
- Javascript Cheat SheetDocument4 pagesJavascript Cheat SheetAttilio FurciNo ratings yet
- HTML Essentials Cheat Sheet PDFDocument1 pageHTML Essentials Cheat Sheet PDFwilliamNo ratings yet
- Corona Virus PDFDocument17 pagesCorona Virus PDFAnanyaja DebadiptaNo ratings yet
- Tips and Tricks For Navigating YoutubeDocument1 pageTips and Tricks For Navigating YoutubeWilroNo ratings yet
- Pandas PracticeDocument117 pagesPandas PracticeAnanyaja DebadiptaNo ratings yet
- Object DetectionDocument5 pagesObject DetectionAnanyaja DebadiptaNo ratings yet
- Quick Navigation Reading Messages: Go To ContactsDocument1 pageQuick Navigation Reading Messages: Go To ContactsAnanyaja DebadiptaNo ratings yet
- Quick Navigation Reading Messages: Go To ContactsDocument1 pageQuick Navigation Reading Messages: Go To ContactsAnanyaja DebadiptaNo ratings yet
- Blast Disease Detection With ML and IP in Cloud - OldDocument48 pagesBlast Disease Detection With ML and IP in Cloud - OldAnanyaja DebadiptaNo ratings yet
- Face Recognition - Understanding LBPH Algorithm - Towards Data ScienceDocument8 pagesFace Recognition - Understanding LBPH Algorithm - Towards Data ScienceAnanyaja DebadiptaNo ratings yet
- Blast Disease Detection With ML and IP in CloudDocument48 pagesBlast Disease Detection With ML and IP in CloudAnanyaja DebadiptaNo ratings yet
- Image SegmentationDocument31 pagesImage SegmentationAnanyaja DebadiptaNo ratings yet
- Blast Disease Detection With ML and IP in CloudDocument48 pagesBlast Disease Detection With ML and IP in CloudAnanyaja DebadiptaNo ratings yet
- NumpyDocument23 pagesNumpyAnanyaja DebadiptaNo ratings yet
- A PROJECT REPORT Submitted by Extracti oDocument44 pagesA PROJECT REPORT Submitted by Extracti oAnanyaja DebadiptaNo ratings yet
- Ec Lab PDFDocument60 pagesEc Lab PDFkrishgkkd3339No ratings yet
- Department of Electronics & Telecommunication Engineering Teaching Plan (5 Sem ENTC) Name of The Teacher: Prof. BISHNU PRIYA SAMALDocument2 pagesDepartment of Electronics & Telecommunication Engineering Teaching Plan (5 Sem ENTC) Name of The Teacher: Prof. BISHNU PRIYA SAMALAnanyaja DebadiptaNo ratings yet
- Introduction To Networking: Charles SeveranceDocument119 pagesIntroduction To Networking: Charles SeveranceShailendra ShaelNo ratings yet
- Enlightenment Life The Way It Is SadhguruDocument83 pagesEnlightenment Life The Way It Is Sadhgurushivasun1100% (2)
- Predicting Bad Commits: Finding Bugs by Learning Their Socio-Organizational PatternsDocument8 pagesPredicting Bad Commits: Finding Bugs by Learning Their Socio-Organizational PatternsbhargavNo ratings yet
- Fakespotter: A Simple Yet Robust Baseline For Spotting Ai-Synthesized Fake FacesDocument8 pagesFakespotter: A Simple Yet Robust Baseline For Spotting Ai-Synthesized Fake FacesAmol SinhaNo ratings yet
- Walidd Score, A New Tool To Diagnose Dysmenorrhea and Predict Medical Leave in University StudentsDocument11 pagesWalidd Score, A New Tool To Diagnose Dysmenorrhea and Predict Medical Leave in University Studentsxavi5_5No ratings yet
- HUang, 2008 D-39Document12 pagesHUang, 2008 D-39Fadel TrianzahNo ratings yet
- B.N.N College, Bhiwandi Department of Information Technology Subject: Business Intelligence Questions BankDocument49 pagesB.N.N College, Bhiwandi Department of Information Technology Subject: Business Intelligence Questions BankYohan MalshikaNo ratings yet
- ML Lab Programs PDFDocument15 pagesML Lab Programs PDFRavi KiranNo ratings yet
- Cheatsheet Machine Learning Tips and Tricks PDFDocument2 pagesCheatsheet Machine Learning Tips and Tricks PDFAshwini NatesanNo ratings yet
- Analysis of Imbalanced Classification Algorithms A Perspective ViewDocument5 pagesAnalysis of Imbalanced Classification Algorithms A Perspective ViewEditor IJTSRDNo ratings yet
- A Student Grouping Method For Massive Online CollaborativeDocument16 pagesA Student Grouping Method For Massive Online CollaborativeNi Nyoman ParwatiNo ratings yet
- Predictive - Modelling - Project - PDF 1Document31 pagesPredictive - Modelling - Project - PDF 1Shiva KumarNo ratings yet
- ML Paper 3Document33 pagesML Paper 3lydiaNo ratings yet
- Accelerometer Data Collection and Processing Criteria To AssessDocument25 pagesAccelerometer Data Collection and Processing Criteria To AssessBJNo ratings yet
- Predicting Credit Risk of Financial Firms in India Using AI-based ML Approaches A Study of Nifty 50 FirmsDocument11 pagesPredicting Credit Risk of Financial Firms in India Using AI-based ML Approaches A Study of Nifty 50 FirmsB. Hari Babu Assistant Professor, Dept. of Business ManagementNo ratings yet
- The Psychometric Properties of The Gilliam AutismDocument14 pagesThe Psychometric Properties of The Gilliam AutismJuan Alberto Veras VelozNo ratings yet
- Handling Imbalanced Data: SMOTE vs. Random UndersamplingDocument4 pagesHandling Imbalanced Data: SMOTE vs. Random UndersamplingAnonymous kw8Yrp0R5rNo ratings yet
- Evaluation Metrics:: Confusion MatrixDocument7 pagesEvaluation Metrics:: Confusion MatrixNithya PrasathNo ratings yet
- BrainNet A Multi-Person Brain-to-Brain Interface FDocument12 pagesBrainNet A Multi-Person Brain-to-Brain Interface FPedro Henrique SenaNo ratings yet
- Rachmat Belgi Saputra - 010.06.005 - New Trauma and Injury Severity Score (TRISS) Adjustment For Survival Prediction - Journal DR DudutDocument6 pagesRachmat Belgi Saputra - 010.06.005 - New Trauma and Injury Severity Score (TRISS) Adjustment For Survival Prediction - Journal DR DudutRachmat B SaputraNo ratings yet
- SMEs Credit Risk Modelling For PDFDocument270 pagesSMEs Credit Risk Modelling For PDFLjiljana SorakNo ratings yet
- PDFDocument22 pagesPDFUmmeHaniAsifNo ratings yet
- Detection: R.G. GallagerDocument18 pagesDetection: R.G. GallagerSyed Muhammad Ashfaq AshrafNo ratings yet
- A New Point-Of-Care Test For The Rapid Detection of Urinary Tract InfectionsDocument8 pagesA New Point-Of-Care Test For The Rapid Detection of Urinary Tract InfectionsAntika CahyatiNo ratings yet
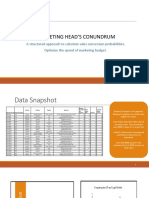
- Marketing Head'S ConundrumDocument16 pagesMarketing Head'S ConundrumUTKARSH PABALENo ratings yet
- Predictive Validity of The Post Partum Depression Predictors Inventory Revised PDFDocument6 pagesPredictive Validity of The Post Partum Depression Predictors Inventory Revised PDFAnonymous jmc9IzFNo ratings yet
- Logistic Regression Quiz SolvedDocument4 pagesLogistic Regression Quiz SolvedRohit Yadav100% (1)
- A Triangle Area Based Nearest Neighbors Approach To Intrusion DetectionDocument8 pagesA Triangle Area Based Nearest Neighbors Approach To Intrusion DetectionHomeed AlzhraniNo ratings yet
- A Comparison of 1-Regularizion, PCA, KPCA and ICA For Dimensionality Reduction in Logistic RegressionDocument20 pagesA Comparison of 1-Regularizion, PCA, KPCA and ICA For Dimensionality Reduction in Logistic RegressionManole Eduard MihaitaNo ratings yet
- Vertigo Sympton ScaleDocument9 pagesVertigo Sympton ScaleIvan HoNo ratings yet
- Artificial Intelligence-Based Lead Propensity PredictionDocument10 pagesArtificial Intelligence-Based Lead Propensity PredictionIAES IJAINo ratings yet
- An Automatic Determining Food Security Status Machine Learning Based Analysis of Household Survey DataDocument12 pagesAn Automatic Determining Food Security Status Machine Learning Based Analysis of Household Survey DataDr-Umar Ijaz AhmedNo ratings yet