You might also like
- 13-勞工保險(勞工職業災害保險)失能診斷書樣本112 08Document16 pages13-勞工保險(勞工職業災害保險)失能診斷書樣本112 08林樹生No ratings yet
- 13-勞工保險(勞工職業災害保險)失能診斷書樣本111 03Document16 pages13-勞工保險(勞工職業災害保險)失能診斷書樣本111 03Q QNo ratings yet
- 何銘初診醫師掛號 - 中國醫藥大學附設醫院Document3 pages何銘初診醫師掛號 - 中國醫藥大學附設醫院Agus LesmanaNo ratings yet
- 印尼金光集团APP 纸业OKI纸厂二期项目制浆、抄浆车间机电安装工程10,16Document5 pages印尼金光集团APP 纸业OKI纸厂二期项目制浆、抄浆车间机电安装工程10,16arief.cncecNo ratings yet
- 13101531183Document3 pages13101531183徐千淑No ratings yet
- 永安欣生代少儿医疗保险单页 20220601Document6 pages永安欣生代少儿医疗保险单页 20220601julia.lamkakeiNo ratings yet
- 到診人士須知中文版2023年3月 KRSCDocument1 page到診人士須知中文版2023年3月 KRSCTaimanNo ratings yet
- 特殊病房知情同意书Document1 page特殊病房知情同意书averamanggalaNo ratings yet
- 1273 3Document1 page1273 3黃俊端No ratings yet
- 1273 2Document1 page1273 2黃俊端No ratings yet
- Case - Shouldice Hospital - 1684397569092Document10 pagesCase - Shouldice Hospital - 1684397569092张于No ratings yet
- 244b785c-8a9e-48f8-8a02-6ee90f328ac8Document5 pages244b785c-8a9e-48f8-8a02-6ee90f328ac8denghaoran1997No ratings yet
- Public Hospitals Key Statistics During Service Demand SurgeDocument1 pagePublic Hospitals Key Statistics During Service Demand SurgeHKFPNo ratings yet
- 107年延攬旅外專科醫師返鄉服務計畫Document8 pages107年延攬旅外專科醫師返鄉服務計畫國亨鄭No ratings yet
- Notes To Visitors TCDocument3 pagesNotes To Visitors TCleo chiuNo ratings yet
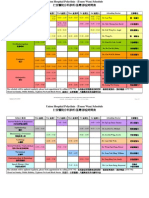
- Union Hospital TST - TimetableDocument2 pagesUnion Hospital TST - Timetable健康生活園Healthy Life GardenNo ratings yet
- 71A0-內科部呼吸治療科 呼吸治療師|中國醫藥大學新竹附設醫院|新竹縣-104 人力銀行Document3 pages71A0-內科部呼吸治療科 呼吸治療師|中國醫藥大學新竹附設醫院|新竹縣-104 人力銀行Jack ChenNo ratings yet
- 醫院評鑑與實驗室認證Document25 pages醫院評鑑與實驗室認證TW RHKLNo ratings yet
- Application For Returning - 155Document1 pageApplication For Returning - 155Saurab SsNo ratings yet
- 34639Document3 pages34639Cheuk Ho TseNo ratings yet
- Union Hospital TWC - TimetableDocument2 pagesUnion Hospital TWC - Timetable健康生活園Healthy Life GardenNo ratings yet
- SodapdfDocument15 pagesSodapdfRidho Sukma WinataNo ratings yet
- 110 初階重症Document5 pages110 初階重症ray510618No ratings yet
- GOPC IVAS A5Leaflet-KEC GBDocument1 pageGOPC IVAS A5Leaflet-KEC GBTsang RebeccaNo ratings yet
- Pre-auth 预授权申请表Document1 pagePre-auth 预授权申请表Anandrao MainkarNo ratings yet
- 805Document17 pages805Ward OxtonNo ratings yet
- 中大學保Document2 pages中大學保q0910670456No ratings yet
- 醫護名詞 P1 12Document12 pages醫護名詞 P1 12Alfred LouNo ratings yet
- 附件 1 4 1 農保身心障礙診斷書 (空白) 10804版 限制列印Document19 pages附件 1 4 1 農保身心障礙診斷書 (空白) 10804版 限制列印王禎翊No ratings yet
- Union Hospital Tko - TimetableDocument3 pagesUnion Hospital Tko - Timetable健康生活園Healthy Life GardenNo ratings yet
- 保險金申請書1120104Document3 pages保險金申請書1120104黃紘志No ratings yet
- 新型冠状病毒 (SARS CoV 2) 核酸筛查报告单 PDFDocument1 page新型冠状病毒 (SARS CoV 2) 核酸筛查报告单 PDFstone HanNo ratings yet
- Health Certificate For Residence ApplicationDocument9 pagesHealth Certificate For Residence Applicationdjun033No ratings yet
- 健康检查申请表Document2 pages健康检查申请表O. NordpolidaNo ratings yet
- Health TaiwanDocument8 pagesHealth TaiwanDinda BazliahNo ratings yet
- 管藥登記證申請書 (新)Document1 page管藥登記證申請書 (新)AnnaNo ratings yet
- Grace Health Centre Family Doctor Waitlist Registration Form 惠恩健康中心家庭医生等候名单报名表Document1 pageGrace Health Centre Family Doctor Waitlist Registration Form 惠恩健康中心家庭医生等候名单报名表forshoppingchristyNo ratings yet
- Hasr 2018 2019 HaoDocument8 pagesHasr 2018 2019 Haotc2tc-399619No ratings yet
- Faq SopDocument3 pagesFaq SopmicsitNo ratings yet
- ,印尼金光集团APP 纸业OKI纸厂二期项目制浆、抄浆车间机电安装工程10,16Document4 pages,印尼金光集团APP 纸业OKI纸厂二期项目制浆、抄浆车间机电安装工程10,16arief.cncecNo ratings yet
- Ams 14 1610Document4 pagesAms 14 1610Vintonius Raffaele PRIMUSNo ratings yet
- 中國 107年度畢業後一般醫學訓練 Pgy 選配簡章Document3 pages中國 107年度畢業後一般醫學訓練 Pgy 選配簡章Jia-PeiWuNo ratings yet
- f2771575-2990-4dfa-8cf7-5c55316ba73bDocument5 pagesf2771575-2990-4dfa-8cf7-5c55316ba73bdenghaoran1997No ratings yet
- 臺中榮民總醫院107年度一般醫學訓練不分科住院醫師訓練招考簡章finalDocument9 pages臺中榮民總醫院107年度一般醫學訓練不分科住院醫師訓練招考簡章finalJia-PeiWuNo ratings yet
- 病症暨失能診斷證明書Document3 pages病症暨失能診斷證明書WayneNo ratings yet
- Ir 1249Document2 pagesIr 1249Vintonius Raffaele PRIMUSNo ratings yet
- 16bc Summary Results PDFDocument166 pages16bc Summary Results PDFVintonius Raffaele PRIMUSNo ratings yet
- M7C83v2 1-ASIADocument214 pagesM7C83v2 1-ASIAVintonius Raffaele PRIMUSNo ratings yet
- TaipoDocument20 pagesTaipoVintonius Raffaele PRIMUSNo ratings yet
- Control Pest Safely C PDFDocument2 pagesControl Pest Safely C PDFVintonius Raffaele PRIMUSNo ratings yet
- Fasp 1a PDFDocument86 pagesFasp 1a PDFVintonius Raffaele PRIMUSNo ratings yet
- Ir 957 AcDocument2 pagesIr 957 AcVintonius Raffaele PRIMUSNo ratings yet
- 本 表 格 的 英 文 版 可 在 本 局 網 頁 www.ird.gov.hk 下 載 或 經 「 表 格 傳 真 服 務 」 (電 話 號 碼 2598 6001) 索 取 。Document4 pages本 表 格 的 英 文 版 可 在 本 局 網 頁 www.ird.gov.hk 下 載 或 經 「 表 格 傳 真 服 務 」 (電 話 號 碼 2598 6001) 索 取 。Vintonius Raffaele PRIMUSNo ratings yet
- Ir 957 CDocument4 pagesIr 957 CVintonius Raffaele PRIMUSNo ratings yet
- Dev20180529 Booklet201804 C PDFDocument78 pagesDev20180529 Booklet201804 C PDFVintonius Raffaele PRIMUSNo ratings yet
- 序言 Foreword: 私人寫字樓 Private Off ice 私人住宅 Private DomesticDocument4 pages序言 Foreword: 私人寫字樓 Private Off ice 私人住宅 Private DomesticVintonius Raffaele PRIMUSNo ratings yet
- Basiclaw Full Text TC PDFDocument167 pagesBasiclaw Full Text TC PDFVintonius Raffaele PRIMUSNo ratings yet
- Ir 6168Document4 pagesIr 6168Vintonius Raffaele PRIMUSNo ratings yet
- Hong Kong Poverty Situation Report 2016 (2017.11.17)Document234 pagesHong Kong Poverty Situation Report 2016 (2017.11.17)Vintonius Raffaele PRIMUSNo ratings yet
- Handout 3 p4 - Activity SheetsDocument1 pageHandout 3 p4 - Activity SheetsVintonius Raffaele PRIMUSNo ratings yet
- Control Pest Safely C PDFDocument2 pagesControl Pest Safely C PDFVintonius Raffaele PRIMUSNo ratings yet
- 私人商業樓宇 Private CommercialDocument6 pages私人商業樓宇 Private CommercialVintonius Raffaele PRIMUSNo ratings yet
- cgn201519458522 PDFDocument15 pagescgn201519458522 PDFVintonius Raffaele PRIMUSNo ratings yet
- 私人寫字樓 (乙級) Private Office (Grade B) : Stock Distribution by AgeDocument4 pages私人寫字樓 (乙級) Private Office (Grade B) : Stock Distribution by AgeVintonius Raffaele PRIMUSNo ratings yet
- 私人寫字樓 (丙級) Private Office (Grade C) : Stock Distribution by AgeDocument4 pages私人寫字樓 (丙級) Private Office (Grade C) : Stock Distribution by AgeVintonius Raffaele PRIMUSNo ratings yet
- TSFS/Review (2019/20)Document2 pagesTSFS/Review (2019/20)Vintonius Raffaele PRIMUSNo ratings yet
- Basiclaw Full Text TCDocument4 pagesBasiclaw Full Text TCVintonius Raffaele PRIMUSNo ratings yet
- 05 PDFDocument56 pages05 PDFVintonius Raffaele PRIMUSNo ratings yet
- 私人工業樓宇 Private IndustrialDocument10 pages私人工業樓宇 Private IndustrialVintonius Raffaele PRIMUSNo ratings yet
- 私人住宅(中 / 小型單位) Private Domestic (Small/Medium Units) : Stock Distribution by AgeDocument4 pages私人住宅(中 / 小型單位) Private Domestic (Small/Medium Units) : Stock Distribution by AgeVintonius Raffaele PRIMUSNo ratings yet
- 03B PDFDocument18 pages03B PDFVintonius Raffaele PRIMUSNo ratings yet
- 私人寫字樓 (甲級) Private Office (Grade A) : Stock Distribution by AgeDocument4 pages私人寫字樓 (甲級) Private Office (Grade A) : Stock Distribution by AgeVintonius Raffaele PRIMUSNo ratings yet
- Plans: 新 界 地 區 New Territories DistrictsDocument3 pagesPlans: 新 界 地 區 New Territories DistrictsVintonius Raffaele PRIMUSNo ratings yet
- 私人寫字樓 (整體) Private Office (Overall) : Stock Distribution by AgeDocument4 pages私人寫字樓 (整體) Private Office (Overall) : Stock Distribution by AgeVintonius Raffaele PRIMUSNo ratings yet
- 序言 Foreword: 私人寫字樓 Private Off ice 私人住宅 Private DomesticDocument4 pages序言 Foreword: 私人寫字樓 Private Off ice 私人住宅 Private DomesticVintonius Raffaele PRIMUSNo ratings yet