You might also like
- Pressure Points-Vital Points and Weak Points of The Human AnatomyDocument1 pagePressure Points-Vital Points and Weak Points of The Human Anatomyjack007xray100% (2)
- Plastic & Hand Surgery in Clinical Practice: Classifications and DefinitionsFrom EverandPlastic & Hand Surgery in Clinical Practice: Classifications and DefinitionsNo ratings yet
- Frog Dissection ADocument7 pagesFrog Dissection AFrances AguinaldoNo ratings yet
- Year 2 NeuroDocument111 pagesYear 2 NeuroShahi GhaniNo ratings yet
- 1-199 PlasticDocument199 pages1-199 Plasticgarfield1No ratings yet
- Reconstructive Surgery - EVANS PDFDocument491 pagesReconstructive Surgery - EVANS PDFOlteanu Ionut100% (3)
- 1.master Techniques in Surgery - Esophageal Surgery, 1E (2014)Document456 pages1.master Techniques in Surgery - Esophageal Surgery, 1E (2014)Raul Micu ChisNo ratings yet
- Guide Golf SwingDocument58 pagesGuide Golf Swingdxdxsrexsresxrexerdx100% (3)
- The Pedicled TRAM Flap in Breast ReconstructionDocument22 pagesThe Pedicled TRAM Flap in Breast ReconstructionJose Mauricio Suarez BecerraNo ratings yet
- University of Louisville Plastic Surgery ManualDocument94 pagesUniversity of Louisville Plastic Surgery ManualBrînduşa CiobanuNo ratings yet
- Geoffrey J. Gladstone, Frank A. Nesi, Evan H. Black - Oculoplastic Surgery Atlas - Cosmetic Facial Surgery-Springer (2018)Document77 pagesGeoffrey J. Gladstone, Frank A. Nesi, Evan H. Black - Oculoplastic Surgery Atlas - Cosmetic Facial Surgery-Springer (2018)DANIEL GIRALDONo ratings yet
- Surgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesFrom EverandSurgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesMelissa Phillips LaPinskaNo ratings yet
- Severe Trauma and Sepsis Organ Damage and Tissue Repair by Xiaobing Fu, Liangming LiuDocument392 pagesSevere Trauma and Sepsis Organ Damage and Tissue Repair by Xiaobing Fu, Liangming LiuDavid Avellaneda TalledoNo ratings yet
- Spinal Cord Anatomy and PathwaysDocument586 pagesSpinal Cord Anatomy and PathwaysarbazNo ratings yet
- Clinical Examination of Acute Adductor InjuriesDocument18 pagesClinical Examination of Acute Adductor Injuriessofianos100% (1)
- Oncoplastic Breast SurgeryDocument20 pagesOncoplastic Breast SurgeryGeorge Yacoup100% (1)
- Neligan Mandible FractureDocument17 pagesNeligan Mandible FractureRibka TheodoraNo ratings yet
- Breast Reconstruction Seminar FinalDocument62 pagesBreast Reconstruction Seminar FinalSumi TranNo ratings yet
- Clinical Anatomy of the Scalp LayersDocument17 pagesClinical Anatomy of the Scalp LayersJustine NyangaresiNo ratings yet
- Regional FlapsDocument55 pagesRegional Flapsswethakari100% (1)
- ABDOMINOPERINEAL RESECTION SURGERYDocument19 pagesABDOMINOPERINEAL RESECTION SURGERYJohnson Mallibago100% (2)
- General Surgery (Must Know)Document93 pagesGeneral Surgery (Must Know)Binit BharatiNo ratings yet
- The Gun Show - Arm WorkoutDocument7 pagesThe Gun Show - Arm Workoutdenby_mNo ratings yet
- Schwartz Chapter 35 Abdominal Wall, Omentum, Mesentery and RetroperitoniumDocument10 pagesSchwartz Chapter 35 Abdominal Wall, Omentum, Mesentery and RetroperitoniumRem Alfelor100% (1)
- Radical Neck DissectionDocument11 pagesRadical Neck DissectionHendry Johannes100% (1)
- Local and Regional Flaps in Head and Neck Cancer / Orthodontic Courses by Indian Dental AcademyDocument56 pagesLocal and Regional Flaps in Head and Neck Cancer / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- All You Need To Know About Vascular SurgeryDocument33 pagesAll You Need To Know About Vascular SurgeryDr. Vinicius MajdalaniNo ratings yet
- Ambulatory Anorectal SurgeryDocument234 pagesAmbulatory Anorectal SurgeryHermina DicuNo ratings yet
- Plastic Surgery Factors Affecting Wound HealingDocument7 pagesPlastic Surgery Factors Affecting Wound HealingRuby Anne RomeroNo ratings yet
- Oncoplastic and Reconstructive BreastDocument14 pagesOncoplastic and Reconstructive BreastYefry Onil Santana Marte100% (1)
- Atlas of Abdominal Wall ReconstructionDocument14 pagesAtlas of Abdominal Wall ReconstructionEmmanuel BarriosNo ratings yet
- SAGES 2018 World Congress Advance ProgramDocument88 pagesSAGES 2018 World Congress Advance Programyos_peace86No ratings yet
- Plastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryDocument23 pagesPlastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryTugce InceNo ratings yet
- Laparoscopic Hepatectomy Atlas and TechniquesDocument327 pagesLaparoscopic Hepatectomy Atlas and TechniquesArassika100% (1)
- Principles of Laparoscopic & Robotic Surgery: Aaquila Sherin Bismi J J Blessy OommanDocument46 pagesPrinciples of Laparoscopic & Robotic Surgery: Aaquila Sherin Bismi J J Blessy OommanAsif AbbasNo ratings yet
- Endocrine Surgery TOM W.J. Lennard Fifth EditionDocument228 pagesEndocrine Surgery TOM W.J. Lennard Fifth EditionSandu AlexandraNo ratings yet
- Gyrokinesis Beginner Series Abs Back StretchesDocument11 pagesGyrokinesis Beginner Series Abs Back StretchesSF Wong100% (2)
- Abdominal Flap PDFDocument67 pagesAbdominal Flap PDFAnonymous Kj8ABF7ANo ratings yet
- Oncoplastic Breast SurgeryDocument27 pagesOncoplastic Breast SurgeryReem Amr El-DafrawiNo ratings yet
- Nasolabial Flap For Oral Cavity ReconstructionDocument10 pagesNasolabial Flap For Oral Cavity ReconstructionJamesNo ratings yet
- FlapsinplasticsurgeryDocument63 pagesFlapsinplasticsurgerysomnathNo ratings yet
- Basic Principles of Plastic SurgeryDocument46 pagesBasic Principles of Plastic SurgeryRAJESH YADAV100% (1)
- Keystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDDocument14 pagesKeystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDlaljadeff12No ratings yet
- Surgery For Recurrent Soft Tissue SarcomaDocument584 pagesSurgery For Recurrent Soft Tissue SarcomaAr-pardo RogerNo ratings yet
- TEPID Breast AugmentationDocument13 pagesTEPID Breast AugmentationbarbpapNo ratings yet
- Tamai Zone 1 Fingertip Amputation: Reconstruction Using A Digital Artery Flap Compared With Microsurgical ReplantationDocument7 pagesTamai Zone 1 Fingertip Amputation: Reconstruction Using A Digital Artery Flap Compared With Microsurgical ReplantationFeliciaDewiNo ratings yet
- Chair Exercises For Older Adults: Many of These Exercises Were Adapted From These SourcesDocument34 pagesChair Exercises For Older Adults: Many of These Exercises Were Adapted From These SourcesthubtendrolmaNo ratings yet
- Oxford Surgery 2018Document14 pagesOxford Surgery 2018Debby rahmadiniNo ratings yet
- BJPS 1984 Cormack Classification of FlapsDocument8 pagesBJPS 1984 Cormack Classification of FlapsS EllurNo ratings yet
- Plastic Surgery 2012Document19 pagesPlastic Surgery 2012khoxNo ratings yet
- Use of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsDocument4 pagesUse of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsPalwasha Malik100% (1)
- The Guide to Breast Reconstruction: Step-By-Step from Mastectomy Through ReconstructionFrom EverandThe Guide to Breast Reconstruction: Step-By-Step from Mastectomy Through ReconstructionRating: 4 out of 5 stars4/5 (1)
- Flaps in Plastic Surgery by DR Roger Christopher GillDocument59 pagesFlaps in Plastic Surgery by DR Roger Christopher GillSemi IqbalNo ratings yet
- Breast Cancer Radiation TherapyDocument439 pagesBreast Cancer Radiation TherapyJuan RivasNo ratings yet
- Guidelines For Laparoscopic (TAPP) and Endoscopic (TEP) Treatment of Inguinal Hernia Surg Endosc 2011Document71 pagesGuidelines For Laparoscopic (TAPP) and Endoscopic (TEP) Treatment of Inguinal Hernia Surg Endosc 2011John Kalaitzis100% (1)
- Flail Chest.Document3 pagesFlail Chest.Irfan ThamrinNo ratings yet
- Neligan Vol 4 Chapter 10 MainDocument20 pagesNeligan Vol 4 Chapter 10 MainisabelNo ratings yet
- Appendiceal Cancer: - 1% of Appendectomies Contain CancerDocument28 pagesAppendiceal Cancer: - 1% of Appendectomies Contain CancerRajendra SoniNo ratings yet
- Essentials CompleteDocument66 pagesEssentials CompleteNovriman LiviaNo ratings yet
- Basic Plastic Surgery Techniques and Principles: How To SutureDocument3 pagesBasic Plastic Surgery Techniques and Principles: How To SutureDarryl BettsNo ratings yet
- Congenital Infiltrating Lipomatosis of The Face Case Report PDFDocument4 pagesCongenital Infiltrating Lipomatosis of The Face Case Report PDFfeli2010No ratings yet
- 2024 Plastic Surgery - Supplementary Applicant HandbookDocument17 pages2024 Plastic Surgery - Supplementary Applicant HandbookwaqbinhassanNo ratings yet
- Flap Selection in Head and Neck Cancer ReconstructionDocument14 pagesFlap Selection in Head and Neck Cancer ReconstructionFerry RusdiansaputraNo ratings yet
- Plastic Surgery ST3 PDFDocument4 pagesPlastic Surgery ST3 PDFM NMNo ratings yet
- Hérnias - Classificação NyhusDocument1 pageHérnias - Classificação NyhusgscapeNo ratings yet
- Faculty: Department of Plastic Surgery B.J.Govt Medical College & Sassoon Hospital, PuneDocument5 pagesFaculty: Department of Plastic Surgery B.J.Govt Medical College & Sassoon Hospital, PuneShubham JoshiNo ratings yet
- ASiT Yearbook 2010, Association of Surgeons in Training PDFDocument131 pagesASiT Yearbook 2010, Association of Surgeons in Training PDFEd FitzgeraldNo ratings yet
- Structural Fat GraftingDocument19 pagesStructural Fat GraftingGautam KalraNo ratings yet
- Suzuki FrameDocument5 pagesSuzuki FrameDimas AryaNo ratings yet
- Skinflaps: Mary Tschoi,, Erik A. Hoy,, Mark S. GranickDocument16 pagesSkinflaps: Mary Tschoi,, Erik A. Hoy,, Mark S. Granickdanico59No ratings yet
- I ST - Vascular SurgeryDocument117 pagesI ST - Vascular SurgeryMohammad_Islam8767% (3)
- Glándula SalivalDocument7 pagesGlándula SalivalGleny SumNo ratings yet
- Resolution of 2nd, 3rd or 4th Interdigital Space Incomplete, Simple Syndactyly Using A Random Vascularity FlapDocument6 pagesResolution of 2nd, 3rd or 4th Interdigital Space Incomplete, Simple Syndactyly Using A Random Vascularity FlapGleny SumNo ratings yet
- PatotidaDocument5 pagesPatotidaGleny SumNo ratings yet
- Steinberg2005 PDFDocument6 pagesSteinberg2005 PDFGleny SumNo ratings yet
- Flaps Selected ReadingsDocument78 pagesFlaps Selected ReadingsIeien MuthmainnahNo ratings yet
- 10 1055 S 0033 1357112 PDFDocument6 pages10 1055 S 0033 1357112 PDFGleny SumNo ratings yet
- Reconstrucción Tejidos BlandosDocument8 pagesReconstrucción Tejidos BlandosGleny SumNo ratings yet
- Glándula SalivalDocument7 pagesGlándula SalivalGleny SumNo ratings yet
- Kim 2013Document11 pagesKim 2013Gleny SumNo ratings yet
- SX OgilvieDocument7 pagesSX OgilvieGleny SumNo ratings yet
- Tumore PfiloidesDocument6 pagesTumore PfiloidesGleny SumNo ratings yet
- Unusual Skin TumorsDocument12 pagesUnusual Skin TumorsGleny SumNo ratings yet
- Gene Expression Modules in Primary Breast Cancers As Risk Factors For Organotropic Patterns of First Metastatic Spread: A Case Control StudyDocument15 pagesGene Expression Modules in Primary Breast Cancers As Risk Factors For Organotropic Patterns of First Metastatic Spread: A Case Control StudyGleny SumNo ratings yet
- Benig Lessions SkinDocument11 pagesBenig Lessions SkinGleny SumNo ratings yet
- Myers - AP Psych Chapter 2 CrosswordDocument2 pagesMyers - AP Psych Chapter 2 CrosswordBrianNo ratings yet
- Chapter 29 The Nervous SystemDocument64 pagesChapter 29 The Nervous SystemAugustus Czar De LeonNo ratings yet
- NAMA: NIM: : Checklist BLOK 3 Pemeriksaan FisikDocument2 pagesNAMA: NIM: : Checklist BLOK 3 Pemeriksaan FisikNovita WulandariNo ratings yet
- Infratemporal FossaDocument12 pagesInfratemporal Fossasuhaira99No ratings yet
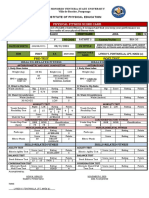
- Don Honorio Ventura State University Physical Fitness Score CardDocument2 pagesDon Honorio Ventura State University Physical Fitness Score CardRed CactusNo ratings yet
- Dr. Faruly Wijaya S. Limba, SPB Rsu BahteramasDocument18 pagesDr. Faruly Wijaya S. Limba, SPB Rsu BahteramasZurezki Andezt YafiieeNo ratings yet
- Shoulder Complex Special TestsDocument30 pagesShoulder Complex Special TestspeawbaNo ratings yet
- The Women's Health Big Book of ExercisesDocument13 pagesThe Women's Health Big Book of ExercisesSylvia GraceNo ratings yet
- Radiography of STN and AbdomenDocument18 pagesRadiography of STN and AbdomenSudil PaudyalNo ratings yet
- Body LinesDocument1 pageBody LinesAnonymous OAEuN9NE1sNo ratings yet
- ONI-CVT#37 Autopsy ReportDocument2 pagesONI-CVT#37 Autopsy Reportbobbob24No ratings yet
- Chapter 8 - Nervous System RP PDFDocument105 pagesChapter 8 - Nervous System RP PDFpizzaNo ratings yet
- Lec8 Sem2 Hnsweek3 20110822Document9 pagesLec8 Sem2 Hnsweek3 20110822Sazter AthiraNo ratings yet
- Classification of dental anomalies and deformitiesDocument15 pagesClassification of dental anomalies and deformitiesAdelina MijaicheNo ratings yet
- Harga RadiologiDocument4 pagesHarga RadiologiyennyNo ratings yet
- General: - Cranial Nerves Same As Spinal ButDocument5 pagesGeneral: - Cranial Nerves Same As Spinal ButjNo ratings yet