You might also like
- International Journal of Cardiology Hypertension: Research PaperDocument6 pagesInternational Journal of Cardiology Hypertension: Research Paperfitria hidayantiNo ratings yet
- Plasma Lipids: Optimal Levels for HealthFrom EverandPlasma Lipids: Optimal Levels for HealthAmerican Health FoundationNo ratings yet
- Chong 2021Document5 pagesChong 2021georgeNo ratings yet
- Reversing Chronic Hypertension Naturally : The Healthy way to Prevent the Silent KillerFrom EverandReversing Chronic Hypertension Naturally : The Healthy way to Prevent the Silent KillerNo ratings yet
- Overview of JNC VI: New Directions in The Management of Hypertension and Cardiovascular RiskDocument8 pagesOverview of JNC VI: New Directions in The Management of Hypertension and Cardiovascular RiskSheila AdiwinataNo ratings yet
- Secondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentFrom EverandSecondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentGeorge A. MansoorNo ratings yet
- Perspective: Management of Hypertension in Patients With Type 2 Diabetes Mellitus: Guidelines Based On Current EvidenceDocument6 pagesPerspective: Management of Hypertension in Patients With Type 2 Diabetes Mellitus: Guidelines Based On Current EvidencethaihavttNo ratings yet
- Hypertension in High Risk African Americans: Current Concepts, Evidence-based Therapeutics and Future ConsiderationsFrom EverandHypertension in High Risk African Americans: Current Concepts, Evidence-based Therapeutics and Future ConsiderationsNo ratings yet
- Diabetes and Hypertension: A Comprehensive Report On Management and The Prevention of Cardiovascular and Renal ComplicationsDocument3 pagesDiabetes and Hypertension: A Comprehensive Report On Management and The Prevention of Cardiovascular and Renal Complicationsrizqi_cepiNo ratings yet
- Home Blood Pressure MonitoringFrom EverandHome Blood Pressure MonitoringGeorge S. StergiouNo ratings yet
- Pencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaDocument7 pagesPencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaFarmasi RSUDNo ratings yet
- s80 FullDocument3 pagess80 FullDiego OrtechoNo ratings yet
- Ioannidis 2017Document2 pagesIoannidis 2017Endang Dwii SuhartiningsihNo ratings yet
- Case Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryDocument9 pagesCase Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryJohn PauloNo ratings yet
- Treatment of HypertensionDocument23 pagesTreatment of HypertensionRABIATUL ADAWIYAHNo ratings yet
- NCM 111 RRL Chapter 2Document5 pagesNCM 111 RRL Chapter 2kyle ibzNo ratings yet
- Hypertensionaha 116 07090 FullDocument2 pagesHypertensionaha 116 07090 FullYanna RizkiaNo ratings yet
- 2016 Article 42 PDFDocument8 pages2016 Article 42 PDFSandhya kumarNo ratings yet
- Primary Prevention of HypertensionDocument7 pagesPrimary Prevention of HypertensioncinthyaaaNo ratings yet
- Case Study: Treating Hypertension in Patients With DiabetesDocument10 pagesCase Study: Treating Hypertension in Patients With Diabetesfirda rydNo ratings yet
- Diabetes and Hypertension: A Comparative Review of Current GuidelinesDocument6 pagesDiabetes and Hypertension: A Comparative Review of Current GuidelineskartikayuanafitriNo ratings yet
- Global Epidemiology CompressedDocument18 pagesGlobal Epidemiology CompressedAdinda Raihana SitorusNo ratings yet
- HHS Public AccessDocument18 pagesHHS Public AccesscarlosNo ratings yet
- HTN Guidelines 1Document12 pagesHTN Guidelines 1lakshminivas PingaliNo ratings yet
- Hypertension Thesis StatementDocument4 pagesHypertension Thesis StatementBuyAPaperOnlineUK100% (2)
- Bmjopen 2016 014736Document6 pagesBmjopen 2016 014736puskesmas patuk satuNo ratings yet
- Diabetesupdate PDFDocument7 pagesDiabetesupdate PDFAndhika Jaya SaputraNo ratings yet
- Trends in Prevalence and Control of Hypertension According To The 2017 American College of Cardiology/American Heart Association (ACC/AHA) GuidelineDocument11 pagesTrends in Prevalence and Control of Hypertension According To The 2017 American College of Cardiology/American Heart Association (ACC/AHA) GuidelineDiana Alvarez SedanoNo ratings yet
- Treatment of Hypertension in Adults With Diabetes: Position StatementDocument3 pagesTreatment of Hypertension in Adults With Diabetes: Position StatementVera WatiNo ratings yet
- Jurnal FarmasiDocument13 pagesJurnal FarmasiDianAyu SuciDwi KusumastutiNo ratings yet
- jnc8 PDFDocument14 pagesjnc8 PDFRizki NovitasariNo ratings yet
- Nihms 1520567Document30 pagesNihms 15205672130020043 RIDHO INAYAHNo ratings yet
- HypertensionDocument3 pagesHypertensionLeirish PabionNo ratings yet
- Katigbak 2018Document9 pagesKatigbak 2018nabilahbilqisNo ratings yet
- Reviews: Global Epidemiology, Health Burden and Effective Interventions For Elevated Blood Pressure and HypertensionDocument18 pagesReviews: Global Epidemiology, Health Burden and Effective Interventions For Elevated Blood Pressure and HypertensionNgô CườngNo ratings yet
- Reviews: Global Epidemiology, Health Burden and Effective Interventions For Elevated Blood Pressure and HypertensionDocument13 pagesReviews: Global Epidemiology, Health Burden and Effective Interventions For Elevated Blood Pressure and HypertensionNgô CườngNo ratings yet
- Top 10 Landmark Studies in HypertensionDocument25 pagesTop 10 Landmark Studies in Hypertensionkaren ordoñezNo ratings yet
- 2020 Hypertension Evolving From Standardized To PrecisionDocument4 pages2020 Hypertension Evolving From Standardized To PrecisionPeter Albeiro Falla CortesNo ratings yet
- Journal of Hypertension: Open Access: Hypertension-A Challenge To Modern MedicineDocument2 pagesJournal of Hypertension: Open Access: Hypertension-A Challenge To Modern MedicineReiner ImranNo ratings yet
- SA Hypertension GuidelinesDocument26 pagesSA Hypertension GuidelinesMaleehaNo ratings yet
- Kidney News Article p29 17Document1 pageKidney News Article p29 17annafebrinaputriNo ratings yet
- Farmacoterapia Actual y Futura en HTADocument15 pagesFarmacoterapia Actual y Futura en HTAGilbertoNo ratings yet
- Management of Hypertension According To JNC 7: by Sandar Kyi, MDDocument27 pagesManagement of Hypertension According To JNC 7: by Sandar Kyi, MDDiana Da SilvaNo ratings yet
- Theassessmentandimportance Ofhypertensioninthedental SettingDocument15 pagesTheassessmentandimportance Ofhypertensioninthedental SettingAngélica Valenzuela AndrighiNo ratings yet
- Correa 2018Document52 pagesCorrea 2018Esteban Matus MuñozNo ratings yet
- Hypertension in Saudi ArabiaDocument8 pagesHypertension in Saudi ArabiaJohn GomezNo ratings yet
- Hypertension Knowledge Heart Healthy Lifestyle Practices and MedDocument8 pagesHypertension Knowledge Heart Healthy Lifestyle Practices and MedAmin KutbiNo ratings yet
- Pi Is 0272638616302645Document9 pagesPi Is 0272638616302645Eko PrasNo ratings yet
- JNC 8 SummaryDocument14 pagesJNC 8 Summaryamm1101No ratings yet
- 1 s2.0 073510979390074B Main PDFDocument2 pages1 s2.0 073510979390074B Main PDFRazali DerausNo ratings yet
- Study of Drug Use in Essential Hypertension and Their ComplianceDocument13 pagesStudy of Drug Use in Essential Hypertension and Their ComplianceRachmat MuhammadNo ratings yet
- 10 1001@jama 2018 16755Document2 pages10 1001@jama 2018 16755Papilionanthae MalindaeNo ratings yet
- Review JNC 8 PDFDocument3 pagesReview JNC 8 PDFandirio7486No ratings yet
- Nihms 567395Document15 pagesNihms 567395fani rudiyantiNo ratings yet
- Dietary Therapy in Hypertension: Clinical TherapeuticsDocument11 pagesDietary Therapy in Hypertension: Clinical TherapeuticsIsti YaniNo ratings yet
- Thiazides and Diabetes: Pharmacist'S Letter / Prescriber'S LetterDocument2 pagesThiazides and Diabetes: Pharmacist'S Letter / Prescriber'S Lettercarramrod2No ratings yet
- Byrd 2019Document22 pagesByrd 2019Miriam TorresNo ratings yet
- JNC 8Document14 pagesJNC 8amiwahyuniNo ratings yet
- 2021 World Health Organization Guideline On PharmaDocument10 pages2021 World Health Organization Guideline On PharmaGiselleNo ratings yet
- Diabetes and Hypertension Physiopathology and Therapeutics: Journal of Human Hypertension May 2000Document7 pagesDiabetes and Hypertension Physiopathology and Therapeutics: Journal of Human Hypertension May 2000chandra9000No ratings yet
- Chronic Hypertension in Pregnancy ACOGDocument25 pagesChronic Hypertension in Pregnancy ACOGJulienni ArvelosNo ratings yet
- Slide Set Pediatric GuidelinesDocument21 pagesSlide Set Pediatric GuidelinesdragonletalNo ratings yet
- Makalah HypertensionDocument6 pagesMakalah HypertensionFatin ZafirahNo ratings yet
- Cilacar CME Final 23-8-2010Document91 pagesCilacar CME Final 23-8-2010Kanchan Pathak100% (1)
- Preoperative Hypertension BJA 2021Document7 pagesPreoperative Hypertension BJA 2021lim sjNo ratings yet
- Philippine National Drug Formulary: Essential Drugs MonographsDocument1,009 pagesPhilippine National Drug Formulary: Essential Drugs MonographsAngelo OstreaNo ratings yet
- MethyldopaDocument5 pagesMethyldopaAnditapitalokaNo ratings yet
- Pharma TablesDocument5 pagesPharma TablesSHRIKANTNo ratings yet
- Emergency Hypertension (Herbesser Injection)Document18 pagesEmergency Hypertension (Herbesser Injection)suho exoNo ratings yet
- Ni Hms 388509Document15 pagesNi Hms 388509Abigail PheiliaNo ratings yet
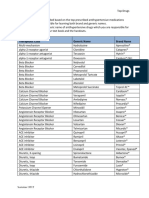
- Top Antihypertensive Drugs Generic-Brand Names PDFDocument1 pageTop Antihypertensive Drugs Generic-Brand Names PDFvidbala0% (1)
- MinoxidilDocument4 pagesMinoxidilapi-3797941100% (1)
- Eclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Document20 pagesEclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Grigore PopaNo ratings yet
- Cardiovascular Pharmacology - Antihypertensive AgentsCardiovascular Pharmacology - Antihypertensive AgentsDocument14 pagesCardiovascular Pharmacology - Antihypertensive AgentsCardiovascular Pharmacology - Antihypertensive AgentsAndySatrioTipunkNo ratings yet
- Epidemiology of Resistant Hypertension in Canada - 2Document7 pagesEpidemiology of Resistant Hypertension in Canada - 2ehaffejeeNo ratings yet
- Treatment of Systemic Hypertension Associated With Kidney DiseaseDocument6 pagesTreatment of Systemic Hypertension Associated With Kidney DiseaseDr.Lázár AttilaNo ratings yet
- Hypertension HerbsDocument30 pagesHypertension HerbsAlexander IvanoffNo ratings yet
- 2nd MB Final Sem Paper-1Document55 pages2nd MB Final Sem Paper-1nirbhikNo ratings yet
- Antihypertensives 2Document6 pagesAntihypertensives 2Manyal Kutin KoakNo ratings yet
- Hypertensive Emergency, El - ShahawyDocument41 pagesHypertensive Emergency, El - ShahawysalwaNo ratings yet
- PHARMA 10 Yrs 2021 Updated TMCPSU MSDMCHDocument15 pagesPHARMA 10 Yrs 2021 Updated TMCPSU MSDMCHNiladri DuttaNo ratings yet
- Telma WriteupDocument3 pagesTelma Writeuph20230845No ratings yet
- Hypertension Prepost Test - Answer KeyDocument3 pagesHypertension Prepost Test - Answer Keyapi-247079964100% (1)
- Nursing Diagnosing (PDAR)Document4 pagesNursing Diagnosing (PDAR)dakieNo ratings yet
- S. Faubel and J. Topf 4 Volume RegulationDocument24 pagesS. Faubel and J. Topf 4 Volume RegulationJoel TopfNo ratings yet
- Pharma 10 Years-1Document15 pagesPharma 10 Years-1Dheeraj Garg100% (1)
- Anti Hypertensive AgentsDocument38 pagesAnti Hypertensive Agentskrishkodal0020No ratings yet
- Amc MCQ PDFDocument48 pagesAmc MCQ PDFSohaib Zafar50% (2)
- HypertensionDocument36 pagesHypertensionRECEPTION AND DIAGNOSTIC CENTER RDC MEDICAL SECTIONNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (32)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4.5 out of 5 stars4.5/5 (6)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingFrom EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingRating: 1 out of 5 stars1/5 (1)