You might also like
- Public Office, Private Interests: Accountability through Income and Asset DisclosureFrom EverandPublic Office, Private Interests: Accountability through Income and Asset DisclosureNo ratings yet
- 04.2 Appendix 2 Conformance Evaluation Record Integrated Preview ENDocument1 page04.2 Appendix 2 Conformance Evaluation Record Integrated Preview ENEmma100% (1)
- QP-STR-02 - Pemeriksaan Penerimaan MaterialDocument6 pagesQP-STR-02 - Pemeriksaan Penerimaan MaterialFendiNo ratings yet
- Management ReviewDocument3 pagesManagement ReviewFendi100% (1)
- Loading and Unloading Checklist May 2021Document2 pagesLoading and Unloading Checklist May 2021Beatrix Uy50% (2)
- Audit Plan ISO 9001Document2 pagesAudit Plan ISO 9001Mokhamad80% (5)
- List of Mandatory Documents Required by ISO 9001Document2 pagesList of Mandatory Documents Required by ISO 9001Rieneke KusmawaningtyasNo ratings yet
- PRE Test Question: Iso 9001 Quality Management SystemDocument4 pagesPRE Test Question: Iso 9001 Quality Management SystemAna Hidayah SyuhadaNo ratings yet
- QMS Audit ChecklistDocument4 pagesQMS Audit ChecklistSyerifaizal Hj. MustaphaNo ratings yet
- The Management Review Process Is As Follows:: 4.0 ProcedureDocument1 pageThe Management Review Process Is As Follows:: 4.0 ProcedureumeshaeroNo ratings yet
- KEY-QMS-05 - F-01 Document Change Request FormDocument1 pageKEY-QMS-05 - F-01 Document Change Request FormMenuka SiwaNo ratings yet
- Continual Improvement ProcedureDocument6 pagesContinual Improvement ProcedureRonald Sarillana100% (1)
- Self Audit Checklist PresentationDocument20 pagesSelf Audit Checklist Presentationnashwan mustafaNo ratings yet
- Irca 106 Audit Log 1Document9 pagesIrca 106 Audit Log 1Huascaran Asesores SacNo ratings yet
- Car Par 001 1Document1 pageCar Par 001 1Andi DumayNo ratings yet
- Audit Plan Matrix ISO 9001:2008Document1 pageAudit Plan Matrix ISO 9001:2008Fatria Rian Ayu100% (1)
- Procedure - Control of Third Party PropertyDocument2 pagesProcedure - Control of Third Party PropertychahiNo ratings yet
- IEC-OP-02 OP For Internal & External CommunicationDocument4 pagesIEC-OP-02 OP For Internal & External CommunicationnomanNo ratings yet
- 17 - Procedure - Control of Records ProcessDocument4 pages17 - Procedure - Control of Records ProcessSaAhRa100% (1)
- Komparasi Iso 9001 Vs Iso 14001 Vs 45001Document2 pagesKomparasi Iso 9001 Vs Iso 14001 Vs 45001Soedarjoto S100% (2)
- Procedure For Control of Customer PropertyDocument4 pagesProcedure For Control of Customer PropertyJobair AlamNo ratings yet
- Tax Audit ChecklistDocument3 pagesTax Audit Checklisthemanth0% (1)
- NCR Records FormDocument10 pagesNCR Records FormTariqMalik100% (1)
- Procedure - Control of Third Party PropertyDocument2 pagesProcedure - Control of Third Party Propertyyudiar2008No ratings yet
- EHQMS Process Audit ReportDocument2 pagesEHQMS Process Audit ReportManuela SavuNo ratings yet
- 3221-C2-V5+V6-CAR Corrective ActionDocument7 pages3221-C2-V5+V6-CAR Corrective ActionIr Azil Awaludin Mohs100% (1)
- PUR-F-SEF - Supplier Evaluation FormDocument1 pagePUR-F-SEF - Supplier Evaluation FormRajkumar PrajapatiNo ratings yet
- Form IA-002A (Audit Plan) (07-13-2012)Document2 pagesForm IA-002A (Audit Plan) (07-13-2012)granburyjohnstevens100% (1)
- Earthquake and Medical Emergency Drill Report - Office 1 (December 14, 2022)Document4 pagesEarthquake and Medical Emergency Drill Report - Office 1 (December 14, 2022)Charles Rommel Tado0% (1)
- Control of Monitoring and Measuring EquipmentDocument3 pagesControl of Monitoring and Measuring EquipmentLinda Setya WatiNo ratings yet
- Irca 106 Audit LogDocument7 pagesIrca 106 Audit LogshaistaNo ratings yet
- Form04 - External Master List of DocumentsDocument1 pageForm04 - External Master List of DocumentsAna Hidayah SyuhadaNo ratings yet
- List of Documents For SEDEX PDFDocument3 pagesList of Documents For SEDEX PDFSunilNo ratings yet
- External Providers Evaluation FormDocument1 pageExternal Providers Evaluation FormISO CERTIFICATION-ROHSNo ratings yet
- Correspondence: ISO 9001:2015/ ISO 14001:2015/ ISO 45001:2018Document3 pagesCorrespondence: ISO 9001:2015/ ISO 14001:2015/ ISO 45001:2018AnkurNo ratings yet
- 010-Audit Report-HatcheryDocument4 pages010-Audit Report-HatcheryAhmed Hassan Shehata100% (1)
- Mandatory Documents and Records Required by ISODocument3 pagesMandatory Documents and Records Required by ISOAli AliNo ratings yet
- QMS 0803 Quality Management System ManualDocument23 pagesQMS 0803 Quality Management System Manualzae nuddin100% (2)
- Otp 2019Document2 pagesOtp 2019Lamtua Purba100% (1)
- ISO 9001 Conformity MatrixDocument3 pagesISO 9001 Conformity Matrixkashifbutty2kNo ratings yet
- Management Review ProcedureDocument1 pageManagement Review ProcedureGaganpreet KaurNo ratings yet
- MRM FormatDocument1 pageMRM FormatGopi AnandNo ratings yet
- QMS Gap ChecklistDocument2 pagesQMS Gap ChecklistIstifadaNo ratings yet
- Corrective Preventive Action FormDocument2 pagesCorrective Preventive Action FormSyed Mujtaba Ali BukhariNo ratings yet
- Section 4Document3 pagesSection 4fuazNo ratings yet
- Description: "Auditor" Review and Acceptance of Corrective Action PlanDocument1 pageDescription: "Auditor" Review and Acceptance of Corrective Action PlanAniekshopNo ratings yet
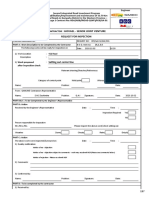
- Corrective Action Form: Owner Logo Contractor LogoDocument1 pageCorrective Action Form: Owner Logo Contractor LogoHoque AnamulNo ratings yet
- Failure Analysis / Corrective Action ReportDocument1 pageFailure Analysis / Corrective Action ReportreiNo ratings yet
- Non Conformance ReportDocument1 pageNon Conformance Reportumar babaNo ratings yet
- QF - 011 - Revised RFADocument3 pagesQF - 011 - Revised RFAAnonymous bIy1lFNo ratings yet
- Non Conformance Report Word TemplateDocument2 pagesNon Conformance Report Word TemplateWilliam JonesNo ratings yet
- 12x 2L Sunstar Loaded From The LineDocument2 pages12x 2L Sunstar Loaded From The LineKgaugelo ShaiNo ratings yet
- Corrective Action ReportDocument1 pageCorrective Action ReportTito GarciaNo ratings yet
- HO CHIEN Enterprise Co., Ltd. Failure Analysis / Corrective Action ReportDocument2 pagesHO CHIEN Enterprise Co., Ltd. Failure Analysis / Corrective Action ReportMaruan MuhammadNo ratings yet
- AV-NC-F01 Non-Conformance Report Iss 1Document1 pageAV-NC-F01 Non-Conformance Report Iss 1Kevin DeLimaNo ratings yet
- Capa Form MjiDocument2 pagesCapa Form MjiSuheriNo ratings yet
- Request For Inspection:: EmployerDocument2 pagesRequest For Inspection:: Employerhovael laboratoryNo ratings yet
- 8D Problem Solving Report: Concern, Title: Order No: Complaint No: Complaint Opening DateDocument2 pages8D Problem Solving Report: Concern, Title: Order No: Complaint No: Complaint Opening DateJean-Marc ValentinNo ratings yet
- 02.03.2020contaminated Sf. Meal Mixed With Uncontaminated MealDocument2 pages02.03.2020contaminated Sf. Meal Mixed With Uncontaminated MealKgaugelo ShaiNo ratings yet
- Request For Inspection:: EmployerDocument2 pagesRequest For Inspection:: Employerhovael laboratoryNo ratings yet
- LABELSLABELSDocument6 pagesLABELSLABELSChinchin Montilla BurdeosNo ratings yet
- CCNAPI Grant Application For SCRN ExamDocument2 pagesCCNAPI Grant Application For SCRN ExamChinchin Montilla BurdeosNo ratings yet
- LSBDAMLA Case DigestsDocument10 pagesLSBDAMLA Case DigestsChinchin Montilla BurdeosNo ratings yet
- 2title PageDocument1 page2title PageChinchin Montilla BurdeosNo ratings yet
- NamesDocument1 pageNamesChinchin Montilla BurdeosNo ratings yet
- Logbooks LabelsDocument1 pageLogbooks LabelsChinchin Montilla BurdeosNo ratings yet
- Recovering After A StrokeDocument17 pagesRecovering After A StrokeTiffany MatthewsNo ratings yet
- Invitation (Repaired)Document1 pageInvitation (Repaired)Chinchin Montilla BurdeosNo ratings yet
- Tagalog MRSDocument5 pagesTagalog MRSChinchin Montilla BurdeosNo ratings yet
- States and Governance Final OutputDocument81 pagesStates and Governance Final OutputChinchin Montilla BurdeosNo ratings yet
- Relationship Between Nursing Care Quality, Nurse Staffing, Nurse Job Satisfaction, Nurse Practice Environment, and Burnout Literature Review PDFDocument7 pagesRelationship Between Nursing Care Quality, Nurse Staffing, Nurse Job Satisfaction, Nurse Practice Environment, and Burnout Literature Review PDFChinchin Montilla BurdeosNo ratings yet
- BDO vs. RepDocument1 pageBDO vs. RepChinchin Montilla Burdeos100% (1)
- States and Governance Final OutputDocument1 pageStates and Governance Final OutputChinchin Montilla BurdeosNo ratings yet
- States and Governance Final OutputDocument81 pagesStates and Governance Final OutputChinchin Montilla BurdeosNo ratings yet
- AMLA CasesDocument32 pagesAMLA CasesChinchin Montilla BurdeosNo ratings yet
- SCRIPTDocument2 pagesSCRIPTChinchin Montilla BurdeosNo ratings yet
- SCRIPTDocument2 pagesSCRIPTChinchin Montilla BurdeosNo ratings yet
- Logbooks LabelsDocument1 pageLogbooks LabelsChinchin Montilla BurdeosNo ratings yet
- Path o Phys OlogyDocument1 pagePath o Phys OlogyChinchin Montilla BurdeosNo ratings yet
- AMLA CasesDocument32 pagesAMLA CasesChinchin Montilla BurdeosNo ratings yet
- AMLA CasesDocument32 pagesAMLA CasesChinchin Montilla BurdeosNo ratings yet
- BDO vs. RepDocument1 pageBDO vs. RepChinchin Montilla Burdeos100% (1)
- Review of LiteratureDocument2 pagesReview of LiteratureChinchin Montilla BurdeosNo ratings yet
- LABELSLABELSDocument6 pagesLABELSLABELSChinchin Montilla BurdeosNo ratings yet
- IntroductionDocument2 pagesIntroductionChinchin Montilla BurdeosNo ratings yet
- FRANCHISEDocument2 pagesFRANCHISEadieNo ratings yet
- Intermediate Accounting 14th Edition Kieso Test BankDocument25 pagesIntermediate Accounting 14th Edition Kieso Test BankReginaGallagherjkrb100% (58)
- A KariozenDocument4 pagesA Kariozenjoseyamil77No ratings yet
- Sec FunctionsDocument105 pagesSec Functionsfolatunde2001No ratings yet
- An 09034Document16 pagesAn 09034lejigeNo ratings yet
- Deal or No Deal Tax 2 Quiz BeeDocument13 pagesDeal or No Deal Tax 2 Quiz BeeRebecca SisonNo ratings yet
- Persona Based Identity and Access ManagementDocument39 pagesPersona Based Identity and Access Managementsneha sureshbabuNo ratings yet
- Annotated Glossary of Terms Used in The Economic Analysis of Agricultural ProjectsDocument140 pagesAnnotated Glossary of Terms Used in The Economic Analysis of Agricultural ProjectsMaria Ines Castelluccio100% (1)
- American Ambulette SchedulesDocument321 pagesAmerican Ambulette SchedulesMNCOOhioNo ratings yet
- Pledge, REM, Antichresis DigestsDocument43 pagesPledge, REM, Antichresis DigestsAnonymous fnlSh4KHIgNo ratings yet
- Dispute Form - Bilingual 2019Document2 pagesDispute Form - Bilingual 2019Kxng MindCtrl OrevaNo ratings yet
- Lessons 1 and 2 Review IBM Coursera TestDocument6 pagesLessons 1 and 2 Review IBM Coursera TestNueNo ratings yet
- "Now 6000 Real-Time Screen Shots With Ten Country Payrolls With Real-Time SAP Blueprint" For Demo Click HereDocument98 pages"Now 6000 Real-Time Screen Shots With Ten Country Payrolls With Real-Time SAP Blueprint" For Demo Click Herevj_aeroNo ratings yet
- Assignment 1.3Document3 pagesAssignment 1.3ZeusNo ratings yet
- Industrial Relations AssignmentDocument13 pagesIndustrial Relations Assignmentrounaq dharNo ratings yet
- Khushboo Kukreja Front PageDocument4 pagesKhushboo Kukreja Front Pagejassi7nishadNo ratings yet
- CH 07Document41 pagesCH 07Mrk KhanNo ratings yet
- BSC Charting Proposal For Banglar JoyjatraDocument12 pagesBSC Charting Proposal For Banglar Joyjatrarabi4457No ratings yet
- FMEA Training v1.1Document78 pagesFMEA Training v1.1Charles Walton100% (1)
- A Guide About Bank AccountsDocument6 pagesA Guide About Bank AccountsHelloprojectNo ratings yet
- Resolution No 003 2020 LoanDocument4 pagesResolution No 003 2020 LoanDexter Bernardo Calanoga TignoNo ratings yet
- Antoine Cited Money LaunderingDocument74 pagesAntoine Cited Money Launderingcorina_maria_eneNo ratings yet
- ch14 ExercisesDocument10 pagesch14 ExercisesAriin TambunanNo ratings yet
- Break Even Point (Bep) Analysis of Tomato Farming Business in Taraitak I Village, Langowan District, Minahasa DistrictDocument8 pagesBreak Even Point (Bep) Analysis of Tomato Farming Business in Taraitak I Village, Langowan District, Minahasa Districtrenita lishandiNo ratings yet
- Online Shopping PDFDocument4 pagesOnline Shopping PDFkeerthanasubramaniNo ratings yet
- Business Plan:: Shannon Lowery Erin Faight Christina Rullo Alec RobertsonDocument12 pagesBusiness Plan:: Shannon Lowery Erin Faight Christina Rullo Alec RobertsonBhavin GhoniyaNo ratings yet
- Obayomi & Sons Farms: Business PlanDocument5 pagesObayomi & Sons Farms: Business PlankissiNo ratings yet
- Chapter 3: Product and Process DesignDocument29 pagesChapter 3: Product and Process DesignGigiNo ratings yet
- Din 11864 / Din 11853: Armaturenwerk Hötensleben GMBHDocument70 pagesDin 11864 / Din 11853: Armaturenwerk Hötensleben GMBHkrisNo ratings yet
- 01 Pengantar SCMDocument46 pages01 Pengantar SCMAdit K. BagaskoroNo ratings yet