You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- COVID 19 Home Care GuidelinesDocument35 pagesCOVID 19 Home Care GuidelinesNeenNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- NBME Question Writing GuidelinesDocument181 pagesNBME Question Writing GuidelinesArsalan N' Tashbee ShabbirNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Role of Physical Education in Promoting Healthy LifestylesDocument42 pagesThe Role of Physical Education in Promoting Healthy Lifestylesjamessabraham2No ratings yet
- How To Prevent Diabetes - A Guide For Those With PrediabetesDocument26 pagesHow To Prevent Diabetes - A Guide For Those With PrediabetesDiabetes CareNo ratings yet
- An Introduction To Spanish For Health Care Workers Communication and Culture, 3e (2010)Document398 pagesAn Introduction To Spanish For Health Care Workers Communication and Culture, 3e (2010)johngaltjeep100% (5)
- Pathology InterviewsDocument138 pagesPathology InterviewsJoanna Marie100% (2)
- Over-the-counter medications for common ailmentsDocument4 pagesOver-the-counter medications for common ailmentsDandi Azmi100% (2)
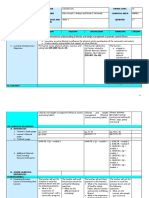
- Daily Lesson Log on Lifestyle and Weight ManagementDocument8 pagesDaily Lesson Log on Lifestyle and Weight ManagementNoel Isaac Maximo100% (2)
- Environmental Modeling and Health Risk AnalysisESTEDocument478 pagesEnvironmental Modeling and Health Risk AnalysisESTESantiago Cardona GalloNo ratings yet
- Full Textbook - CHCCCS011Document62 pagesFull Textbook - CHCCCS011Kabita123 NepzzNo ratings yet
- Report On AganwadiDocument5 pagesReport On AganwadiAkansha JohnNo ratings yet
- NSW Teacher Shortages: June 2021Document22 pagesNSW Teacher Shortages: June 2021NeenNo ratings yet
- PublicHealthMap 50km No5Document1 pagePublicHealthMap 50km No5NeenNo ratings yet
- Road Closures Map NYE 2022Document1 pageRoad Closures Map NYE 2022NeenNo ratings yet
- NSW Teachers Shortages: October 2022Document22 pagesNSW Teachers Shortages: October 2022NeenNo ratings yet
- Gourmet Coast Members FlyerDocument1 pageGourmet Coast Members FlyerNeenNo ratings yet
- Paralympics Day 2Document2 pagesParalympics Day 2NeenNo ratings yet
- Gilmore: February 2016 Map of The Federal Electoral Division ofDocument1 pageGilmore: February 2016 Map of The Federal Electoral Division ofNeenNo ratings yet
- Whitlam: February 2016 Map of The Federal Electoral Division ofDocument1 pageWhitlam: February 2016 Map of The Federal Electoral Division ofNeenNo ratings yet
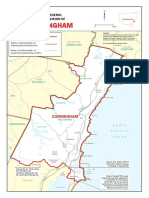
- Cunningham: February 2016 Map of The Federal Electoral Division ofDocument1 pageCunningham: February 2016 Map of The Federal Electoral Division ofNeenNo ratings yet
- Tokyo Paralympics Day 2Document1 pageTokyo Paralympics Day 2NeenNo ratings yet
- CPP - Storm Statement - FVVDocument1 pageCPP - Storm Statement - FVVNeenNo ratings yet
- Managing Mild COVID 19 at Home With Assistance From Your GPDocument26 pagesManaging Mild COVID 19 at Home With Assistance From Your GPNeenNo ratings yet
- Tokyo Paralympics Day 6Document1 pageTokyo Paralympics Day 6NeenNo ratings yet
- Tokyo Paralympics 2021: August 25Document2 pagesTokyo Paralympics 2021: August 25NeenNo ratings yet
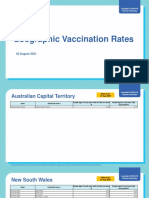
- Covid 19 Vaccination Geographic Vaccination Rates - August 2, 2021Document11 pagesCovid 19 Vaccination Geographic Vaccination Rates - August 2, 2021NeenNo ratings yet
- Bathurst 1000Document1 pageBathurst 1000NeenNo ratings yet
- PublicHealthMap 50km No5Document1 pagePublicHealthMap 50km No5NeenNo ratings yet
- Prepare For FireDocument4 pagesPrepare For FireNeenNo ratings yet
- Fire Equipment, ClothingDocument1 pageFire Equipment, ClothingNeenNo ratings yet
- 27 - Bushfire SeasonDocument2 pages27 - Bushfire SeasonNeenNo ratings yet
- 28 - Bushfire SeasonDocument6 pages28 - Bushfire SeasonNeenNo ratings yet
- Program VIC2021 FA LowresDocument9 pagesProgram VIC2021 FA LowresNeenNo ratings yet
- Fire Evacuation Packing ChecklistDocument1 pageFire Evacuation Packing ChecklistNeenNo ratings yet
- Fire Evacuation Packing ChecklistDocument1 pageFire Evacuation Packing ChecklistNeenNo ratings yet
- Document, Pets and Clothing ChecklistDocument1 pageDocument, Pets and Clothing ChecklistNeenNo ratings yet
- Government Gazette: New South WalesDocument11 pagesGovernment Gazette: New South WalesNeenNo ratings yet
- ALPA Agency Award Submission Criteria V3 2007Document2 pagesALPA Agency Award Submission Criteria V3 2007Kim ChappellNo ratings yet
- Government Gazette: New South WalesDocument11 pagesGovernment Gazette: New South WalesNeenNo ratings yet
- ALPA Agency Award Rules and Conditions V5 2004Document3 pagesALPA Agency Award Rules and Conditions V5 2004Kim ChappellNo ratings yet
- Bu Ning Ahli k3k Mei 22 - Overview-OkDocument34 pagesBu Ning Ahli k3k Mei 22 - Overview-OkArista DianaNo ratings yet
- STRATEGIC ANALYSIS OF BAYBAY RESTAURANTDocument7 pagesSTRATEGIC ANALYSIS OF BAYBAY RESTAURANTAngeline Maquiso SumaoyNo ratings yet
- PE 11 Modules For First Semester 1 1Document30 pagesPE 11 Modules For First Semester 1 1Joseph LapsoNo ratings yet
- Aseptic Practice Recommendations For Circulating Operating Theatre NursesDocument6 pagesAseptic Practice Recommendations For Circulating Operating Theatre NursesJudy-Anne PatricioNo ratings yet
- Parkland StatementDocument2 pagesParkland StatementThe Dallas Morning NewsNo ratings yet
- Problem Statement WORLD Cancer Afflicts All Communities WorldwideDocument30 pagesProblem Statement WORLD Cancer Afflicts All Communities Worldwidesalma0430100% (2)
- Buletin Farmasi 11/2013Document10 pagesBuletin Farmasi 11/2013afiq83No ratings yet
- Antimaleria Drug ModelsDocument33 pagesAntimaleria Drug ModelsMehari AsratNo ratings yet
- SDS AkzoNobelDocument16 pagesSDS AkzoNobelOviedo RocíoNo ratings yet
- Proposal Security Integrated SystemDocument46 pagesProposal Security Integrated SystemIndra Jaya100% (1)
- Overview and Pathophysiology of Gestational Trophoblastic Disease - PresentationDocument222 pagesOverview and Pathophysiology of Gestational Trophoblastic Disease - PresentationTanvir AhmedNo ratings yet
- Project Report On Stress ManagementDocument73 pagesProject Report On Stress ManagementPriya KuttyNo ratings yet
- Go Ms 38 Private Hospital Within and Outside State PDFDocument3 pagesGo Ms 38 Private Hospital Within and Outside State PDFsivaNo ratings yet
- Nutrition Support in Adults NICE Guideline PDFDocument54 pagesNutrition Support in Adults NICE Guideline PDFnewtypeNo ratings yet
- Regional Peacekeepers Collective StrategyDocument17 pagesRegional Peacekeepers Collective StrategyJeremy HarrisNo ratings yet
- Collection, Transportation, Treatment & Disposal of Laboratory WasteDocument51 pagesCollection, Transportation, Treatment & Disposal of Laboratory WasteYuresh TwayanaNo ratings yet
- NitriVer® 3 Nitrite ReagentDocument16 pagesNitriVer® 3 Nitrite ReagentMark KuttinNo ratings yet
- Classroom Nutritional Status ReportDocument2 pagesClassroom Nutritional Status ReportEden PingliNo ratings yet
- MUET ReflectionDocument2 pagesMUET ReflectionNurul NajihahNo ratings yet
- IJM Safety Conference Paper Summarizes NADOPOD 2004 Reporting RegulationsDocument1 pageIJM Safety Conference Paper Summarizes NADOPOD 2004 Reporting RegulationsKay AayNo ratings yet